Introduction
This is a surgical emergency and needs to be diagnosed early so that treatment can be given early with the least complications. Intussusception is the telescoping of the proximal intestine inside the distal intestine.
Background: The gastrointestinal tract consists of the stomach, small intestine, and large intestine. Intussusception occurs when the proximal intestine telescopes into the distal intestine. As seen, the intestine has a mesentery that supplies blood to the intestine. When this telescoping occurs, a number of events can occur in a sequence that gives rise to an emergency. First, the intestine within the intestine compromises the lumen of the intestine, leads to a narrowing and obstruction of the bowel. Since the mesentery gets pulled in along with the intestine, the veins in the mesentery get compressed between the two segments of the intestine-outer and inner. This gradually leads to venous outflow obstruction and congestion of blood in the bowel. Unrelieved, the arteries supplying blood to that intestine which inside gets compressed and blood supply to the inner bowel gets shut off and leads to gangrene. The exact etiology of why this happens is not very well understood, but, usually, there is like a leading point that initiates the process like a polyp in the intestine, enlarged patch of lymphatics in the bowel. Also may be seen to occur soon after a viral cold or diarrhea in a child of viral origin.
Presentation
This is a condition commonly found in infants about 6 - 9 months old "just after starting weaning from breastfeeds to top feeds. It can occur in either sex, usually chubby children, who are otherwise healthy. The infant will classically present with sudden attacks of colicky abdominal pain with screaming, drawing up of the legs, crying. The child may have a small vomit, may later become suddenly quiet. This is followed by another attack of severe pain. Gradually the abdomen starts to distend, the vomiting may recur and turn from white to green(bilious). Initially, the child may pass normal stool, but later may pass a stool that is a mixture of mucus, blood. This last symptom can shake the parent's confidence and they run to the doctor. Examination by the doctor of this child when quiet, may reveal a mass in the abdomen" sausage-shaped usually upper midline above the umbilicus. This lump is due to the intussuscepted bowel loops. The history of the pain and screams is very suggestive of this condition, especially given the age of the child.
Investigations
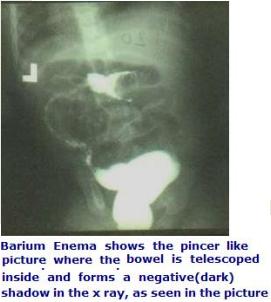
In a suspected case of intussusception, Ultrasonography is ideal. This will pick up the mass of the intestines that will look like concentric circles within each other called target sign. The diagnosis can be very accurate. With the addition of color Doppler study simultaneously, the blood flow to the segments of the intestine can be seen and gangrene can be picked up. An older method of diagnosis is a Barium Enema. In this, a tube is inserted into the rectum of the child and liquid white Barium is injected into the child and allowed to flow and seen on the x-ray machine. A negative shadow is seen and the barium flows like a pincer around the shadow in the center. The diagnosis can be confirmed by these methods.
Figure: Ba enema showing intussusception
Treatment
Nowadays, the therapy is combined with the diagnosis. In the case of Barium Enema, it is given under an x-ray image intensifier through a can placed at 3 feet above the child. The barium flows with the pressure of gravity and not hand force. This hydrostatic force of the liquid barium itself after making a diagnosis begins reducing the intussusception. This occurs as the liquid pushes the proximal inner intestine backward and out of the distal bowel until the entire intussusception is reduced. This procedure is done by the combination of the pediatric surgeon and the radiologist. A very similar procedure can be done under Sonography control and the use of Normal Saline liquid. The advantage is that in this there is no exposure of the child to radiation. Completion of the process can be visualized in both procedures and repeat sonography after 8 hours will confirm no residual or recurrent intussusception is present. In this procedure, the child remains in the hospital for 2 days, there is no surgery, no scar, no operative pain and is back on oral feeds in 48 hours.
Figure: Progressive reduction of the Intussusception

Figure a: Progressive reduction of the Intussusception

Figure b: Progressive reduction of the Intussusception

Intussusception - Surgery
However, in some cases that are brought to the doctor late, or where these procedures fail, the option is to do an open surgery under general anesthesia. The child abdomen is opened and the bowel is inspected, and the intussusception area is localized, and the manual reduction is begun if possible the intestines are checked for gangrene or perforation after reduction and if normal the abdomen is closed. If the intussusception cannot be reduced or there is gangrene of the intestine, such intestine has to be removed and the remaining parts of the intestines are joined together and then the abdomen is closed. These children are very toxic soon after surgery and may go into generalized sepsis and require high antibiotics for a long time of 10 days, along with intravenous fluids no oral intake for 7 days, and a long period of hospitalization.
Figure: Intussusception leading to gangrene

Complications
Nonreducibility by the hydrostatic method entails open surgery. Rare complications of the hydrostatic method are perforation of the intestine, reduction of the potentially unhealthy intestine. Open surgery has its usual complications like wound infection, blood septicemia, leakage of the joining(anastomosis) intestinal segments, perforation of the intestine that looked healthy at surgery a few days after closure. A careful and close follow up with the doctor after discharge for about 15 days is essential to avoid or early detection of these complications. Recurrence of the intussusception can occur after either procedure open or closed.