Inês Ferreira Costa
1, Inês Araújo Oliveira
1, Joana Cardoso
2, Catarina Matos de Figueiredo
21Department of Pediatrics, Unidade Local de Saúde de Santo António, Porto, Portugal,
2Department of Pediatrics, Unidade Local de Saúde de Entre Douro e Vouga, Santa Maria da Feira, Portugal
Address for Correspondence: Inês Ferreira da Costa, Rua dos Bombeiros Voluntários São Mamede de Infesta, 4465-262 São Mamede de Infesta, Porto, Portugal.
Email: inesfcosta6@gmail.com
Keywords : Spontaneous pneumomediastinum, Pediatrics, Subcutaneous emphysema.
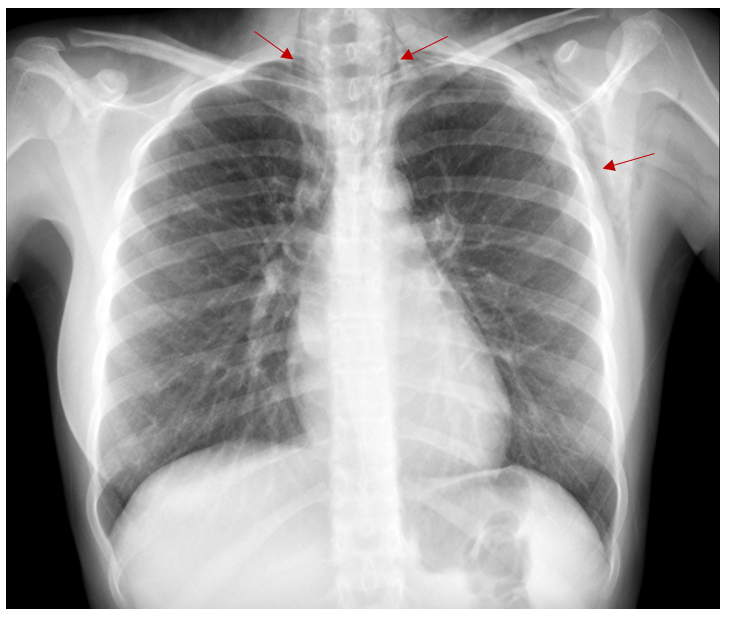
Question: A 14-year-old girl, with a previous history of controlled asthma without any chronic medication, was admitted to the emergency department with dyspnea, neck and chest pain. Without history of trauma, she only mentioned that a friend jumped on her back a few hours earlier. The primary examination revealed a blood pressure of 109/68 mmHg (50th percentile), heart rate of 89 beats/min and oxygen saturation of 97%, with palpable crepitus in the anterior chest wall and neck and diminished breath sounds in pulmonary auscultation. The rest of the physical examination was unremarkable. Electrocardiography shown normal sinus rhythm without QTc prolongation or axis deviation. Chest X-ray is shown on Figure 1.
Figure 1. Chest X-ray revealing pneumomediastinum and bilateral subcutaneous emphysema, over the neck and left side of chest wall (red arrows).