Andre Costa Silva1, Licinia Lima2, Bernardete Rodrigues2, Arnado Rêgo2, Carla Dias2, Isabel Soro2, Dalila Rocha2.
1Department of Pediatrics, Unidade Local de Saúde Alto Minho, Povoa De Varzim, Portugal,
2ULSAM, Hospital Santa Luzia, Viana Castelo, Viana, Portugal.
ADDRESS FOR CORRESPONDENCE
Andre Costa Silva, Av Mouzinho de Albuquerque 59 Póvoa de Varzim, Porto, Portugal.
Email: andrecostaesilva1@gmail.com. | | Abstract | Background: Meconium peritonitis is a rare condition characterized by sterile chemical peritonitis resulting from intrauterine bowel perforation. An even rarer entity occurs when meconium reaches the paratesticular soft tissue through a patent processus vaginalis, meconium periorchitis.
Case presentation: We hereby report a rare case of meconium periorchitis diagnosed following the investigation for a testicular mass in newborn. The diagnosis was confirmed by laparoscopic surgery. Concurrently alpha-1 antitrypsin deficiency is also determined on the midst the investigation.
Conclusion: When investigating a testicular mass in a newborn, a variety of diagnosis should be considered by clinicians including meconium periorchitis. Ultrasonography represents the gold-standard imaging technique due to its ability to differentiate between the extratesticular and intratesticular masses.
| | | | Keywords | | Hydrocele, Meconium peritonitis, Meconium periorchitis, Alpha-1 antitrypsin deficiency. | | | | Introduction | Meconium leakage into the peritoneal cavity induces meconium peritonitis (MP), a sterile chemical peritonitis. It is rare condition with a 1 in 30,000 birth incidence rate.1,2 MP was thought to be a lethal illness between 1950 and 1960, with a death rate of 80% to 90%. Since then, a marked improvement in the survival rate—up to 80%—has been noted. This could arise from advancements in prenatal diagnosis methods and effective early intervention.2
Although the etiology of MP is not fully understood, some theories regarding the perforation mechanism have been put forth. According to some writers, a reduction in blood flow to the mesentery artery may produce mucosal necrosis, which may cause bowel obstruction; a further reduction in mesenteric blood flow may result in necrosis and intestinal wall perforation. However, ischemia is not the only factor that contributes to intestinal wall perforation during the fetal stages. In addition to meconium plugs, extramural conditions like hernia, band and volvulus can also elicit gut obstruction, leading to a perforation.2
Possible causes of MP1,2,3 are listed in Table 1.
Table 1. Major causes of MP.
| Vascular occlusion |
| Meconium ileus* |
| Internal hernia |
| Intussusception |
| Volvulus |
| Hirschsprung disease |
| Intrauterine appendiceal rupture |
| Meckel diverticulum |
| Imperforate anus |
*Causes of meconium ileus: Cystic fibrosis, ileocecal atresia, functional consequence of prematurity pancreatic duct stenosis and partial pancreatic aplasia.
Meconium ascites develops as a result of meconium leakage into the peritoneal cavity following intestinal perforation. A severe inflammatory response brought on by the extruded meconium results in calcium depositing on the abdominal walls and other intra-abdominal tissues.3 A fibrous wall may grow around the meconium concentration, establishing a pseudocyst, if the perforation happens early enough, before to delivery and the leakage persists over a significant amount of time. Predisposing factors include infections (mainly cytomegalovirus infection and parvovirus B19 or genetics, with cystic fibrosis accounting for 20-40 % of all cases of MP.1,2,3)
Meconium periorchitis or MPO, is a rare condition in which meconium enters the paratesticular soft tissue through a patent processus vaginalis and causes an inflammatory response. It can appear at birth as a soft hydrocele, a scrotal enlargement or a discoloration incorrectly attributed to birth trauma. As the meconium calcifies, the scrotal mass that develops over the course of weeks or months, becomes harder.4,5 Scrotal mass at birth presents a broad differential diagnosis as summarized in Table 2.4,6,7,8
Table 2. Differential diagnosis of scrotal mass.
| With calcifications |
Without calcifications |
| Sertoli tumors |
Hydrocele (simple) |
| Gonadoblastoma |
Inguinal hernia |
| Teratoma |
|
| Volvulus |
| Meconium periorchitis |
| Metastatic neuroblastoma |
| Testicular torsion followed by hemorrhagic infarction |
Regarding MPO diagnosis, imaging by scrotal and abdominal ultrasonography is the gold standard.7 It has been suggested that calcifications in the scrotum and abdomen are diagnostic. However, the majority of situations in the literature do not list these calcifications in either the scrotum or the abdomen.8
| | | | Case Report | We hereby present the case of a newborn, born after an uneventful pregnancy, with the exception of the third trimester ultrasound which displayed intrascrotal disperse calcifications, no reference to other findings, specifically abdominal lesions. Clinical examination of the newborn on his first day of life revealed bilateral enlargement of the testicles alongside with a darker coloration of the scrotum. Palpation was “stony” and transillumination test was negative as depicted on Figure 1.
Figure 1. Testicular enlargement and negative transillumination of scrotum.

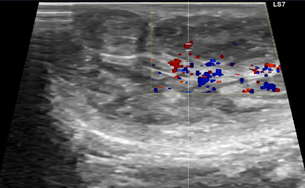
Ultrasound with doppler confirmed ecogenic and heterogeneous material in both scrotal sacs, including several calcific formations (Figure 2) and no signs of vascular compromise (Figure 3).
Figure 2. Testicular ultrasonography of the newborn showing several small calcific hyperechoic formations (arrows).
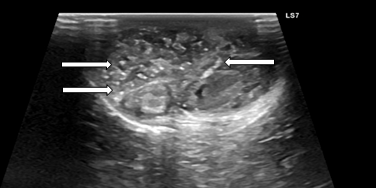
Figure 3. Testicular ultrasonography with doppler of the newborn showing no vascular compromise.
Both testicles had normal size and were symmetrical. Blood tests were performed at day 2. Full blood count, serum C-reactive protein, alpha-fetoprotein levels and b-human chorionic gonadotrophin (b-HCG) were all within age-appropriate age. Total and direct bilirubin were respectively 4.47 and 3.06 mg/dl. The days that followed the newborn was submitted to an abdominal ultrasound and radiography, both suggesting peritoneal calcifications. When combined, these results point out strongly to a diagnostic of meconium periorchitis,7,8 that is an inflammation on the scrotal sac as a result of a peritonitis process that crossed the peritoneal-vaginal duct.
Clinically the newborn was found to be more hypoactive and feeding worse on day 4 and 5 after birth. Pediatric surgery was then consulted and based on clinical and radiographic findings decided to perform an exploratory laparotomy. Multiple meconial concretions and hard meconial pseudocysts were found and removed confirming the diagnosis of meconium periorchitis. Also, a prophylactic appendicectomy was performed. It was decided not to perform bilateral orchidopexy, instead a “wait and see” approach with recurrent evaluations.
Cystic fibrosis was tested and both metabolic and genetic tests were negative for multiple mutations of CFTR gene. Post-surgically, the new-born evolved with no significant complications but the cholestasis parameters remained high. Infants with meconium ileus alone are at an increased risk of neonatal cholestasis. Further studies showed alpha 1 antitrypsin deficiency (AAT deficiency). Genetic tests followed for alpha 1 antitrypsin deficiency and SZ phenotype was identified. There is only one case described on literature with both alpha 1 antitrypsin deficiency and meconium ileus, in which, meconium ileus was associated with cystic fibrosis.8 | | | | Discussion | When bowel wall is perforated, usually in the late fetal or early postnatal period, meconium leakages into the peritoneal cavity, resulting in meconium peritonitis. Table 1 lists the etiologies of MP, including mesenteric vascular insufficiency, volvulus and meconium ileus. If the perforated gut wall heals, the “why” and “where” of the perforation might not be visible or acknowledgeable. Meconium passing through the patent processus vaginalis can induce MPO and the mass-like lesion develops as a result of an inflammatory response to the meconium in the scrotal sac. The meconium ileus is the most typical reason for obstruction. According to most statistics, cystic fibrosis accounts for over 80% of cases of meconium ileus, which causes the meconium to thicken even more due to a lack of pancreatic enzymes. Therefore, screening patients for cystic fibrosis in the context of MPO should always be considered. In a recent assessment, up to 9% of MPO patients had cystic fibrosis diagnosed. In contrast, in MP, cystic fibrosis is discovered in up to 20-40% of patients.8 Regarding the clinical history, it should be remembered that cocaine and non-steroidal anti-inflammatory medicines (NSAIDs) consumption by the mother is known to result in intestinal ischemia and should also be taken into consideration in the differential for a newborn who has signs of in utero intestinal perforation.4,8 Due to its capacity to distinguish between extratesticular and intratesticular masses, ultrasonography is the imaging method of choice. We know that the majority of extratesticular lesions are benign, whereas the majority of intratesticular lesions are malignant. As to abdominal radiographs, they can be used to identify calcifications and significantly support the theory that meconium periorchitis is present. Simultaneous scrotal and abdominal calcifications virtually make up the diagnosis of MPO. Recent research has connected AAT deficiency to ANCA-associated vasculitis, chronic renal disease, diabetes and metabolic changes, including lower serum triglyceride levels.13 Excess of neutrophil elastase determined by alpha 1 antitrypsin deficiency leads to structural damage and consequently emphysema on the lungs. A possible similar mechanism could be responsible for the colonic/ileal perforation and the occurrence of meconium peritonitis/periorchitis. Further studies on this matter are needed.
Learning Points:
- Meconium periorchitis, an uncommon condition, is brought on by meconium leakage into the scrotal sac, which results in sterile inflammation.
- Ultrasonography represents the gold standard imaging technique in testicular enlargement, due to its ability to differentiate between the extratesticular and intratesticular masses.
- Simultaneous scrotal and abdominal calcifications virtually make up the diagnosis of MPO.
- While in asymptomatic neonates, conservative treatment/ surveillance is enough, severely ill patients are in need for urgent surgical intervention.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Shiri Shinar et al, Fetal Meconium Peritonitis - Prenatal Findings and Postnatal Outcome: A Case Series, Systematic Review, and Meta-Analysis, Ultraschall Med, 2020 Jun 23. DOI: 10.1055/a-1194-4363. [CrossRef] [PubMed]
- So Hyun Nam et al, Experience with meconium peritonitis, Journal of Pediatric Surgery, 2007. https://doi.org/10.1016/j.jpedsurg.2007.07.006. [CrossRef] [PubMed]
- Reynolds, E., Douglass, B. & Bleacher, J. Meconium Peritonitis. J Perinatol 20, 193-195 2000. https://doi.org/10.1038/sj.jp.7200287. [CrossRef] [PubMed]
- Pamela Acosta et al, Meconium periorchitis. A case report, Arch Argent Pediatr 2015 http://dx.doi.org/10.5546/aap.2015.e330. [CrossRef]
- Alanbuki AH, Bandi A, Blackford N. Meconium periorchitis: A case report and literature review. Can Urol Assoc J. 2013;7:E495-8. DOI: 10.5489/cuaj.316. [CrossRef] [PubMed] [PMC free article]
- Algaba F, Mikuz G, Boccon-Gibod L, et al. Pseudoneoplastic lesions of the testis and paratesticular structures. Virchows Archiv. 2007;451(6):987-997. DOI: 10.1007/s00428-007-0502-8. [CrossRef] [PubMed] [PMC free article]
- Regev RH, Markovich O, Arnon S, Bauer S, Dolfin T, Litmanovitz I. Meconium periorchitis: intrauterine diagnosis and neonatal outcome: case reports and review of the literature. J Perinatol. 2009 Aug;29(8):585-7. doi: 10.1038/jp.2009.15. PMID: 19638993. [CrossRef] [PubMed]
- Shapira R, Hadzic N, Francavilla R, Koukulis G, Price JF, Mieli-Vergani G. Retrospective review of cystic fibrosis presenting as infantile liver disease. Arch Dis Child. 1999 Aug;81(2):125-8. doi: 10.1136/adc.81.2.125. PMID: 10490518; PMCID: PMC1718019. [CrossRef] [PubMed] [PMC free article]
DOI: https://doi.org/10.7199/ped.oncall.2026.3
|
| Cite this article as: | | Silva A C, Lima L, Rodrigues B, Rêgo A, Dias C, Soro I, Rocha D. Newborn with a rare cause for testicular enlargement. Pediatr Oncall J. 2026;23: 39-41. doi: 10.7199/ped.oncall.2026.3 |
|