Saugat Ghosh, Kheya Ghosh Uttam, Priti Khemka, Rafikul Islam, Shabana Kabir.
Institute of Child Health, Kolkata, India.
ADDRESS FOR CORRESPONDENCE
Saugat Ghosh, Institute of Child Health, Biresh Guha Street, Park Circus, Kolkata, 700017, India.
Email: ghoshsaugat6@gmail.com | | Abstract | | Neonatal ascites is a rare condition characterized by the accumulation of fluid in the peritoneal cavity of a newborn. It is caused by a number of etiologies, the urogenital anomailies are most common cause of neonatal ascites. GIT causes and TORCH infections are the next common causes. The management and prognosis depends on the etiology There is scarcity of literature in this subject. About 5 cases of neonatal ascitis, admitted in last 3 years in our institute, was retrospectively studied. The 5 cases include 2 chylous ascites, 1 urinary ascites, 1 ascites due to liver failure and galactosemia and 1 meconium peritonitis. | | | | Keywords | Ascites, Neonate, Galactosemia, Chylous ascitis, Urinary ascitis
| | | | Introduction | Neonatal ascites is a rare condition characterized by the accumulation of fluid in the peritoneal cavity of a newborn. It is caused by a number of etiologies which include diseases of genitourinary system, gastrointestinal system, cardiac disease, hepatic disease, TORCH or parvovirus infection, chylous, ovarian cause, inborn error of metabolism and idiopathic.1 The urogenital anomailies are most common cause of neonatal ascites. GIT causes and TORCH infection are the next common causes.2, Neonatal ascites is a rare problem and there is scarcity of literature in this subject,5 cases of neonatal ascitis, admitted in last 3 years in our institute, was retrospectively studied and is described below:
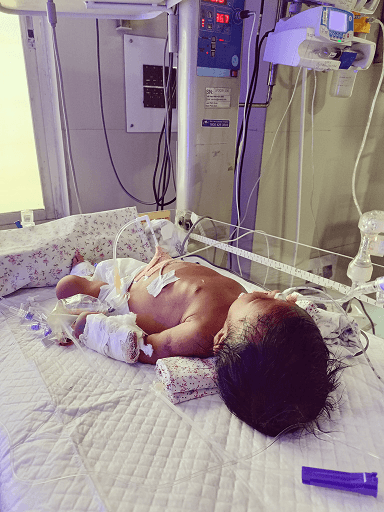
Case 1: A term newborn, on exclusive breastfed had 1 episode of hypoglycaemic seizure on day 7 of life. He was treated in a local hospital and cause of hypoglycaemia was suspected due to poor feed intake. The baby presented later on day 28 of life with significant weight loss, conjugated jaundice and ascites. Diagnostic and therapeutic ascitic tap was done, cell count-25 cells/cu mm with protein 1.8 gm/dl. LFT and PT, APTT was severely deranged with INR>2 persistently. Urine reducing substance was positive so soya milk formula was started but no significant improvement. There was proteinuria and passage of urobilinogen and bilirubin in urine. After 5 days of admission baby developed sudden anuria so peritoneal dialysis was started but there was no significant improvement. USG KUB was suggestive of raised echogenecity of bilateral kidney. Blood culture was negative but there was Acinetobactor growth in bal. Urine succinylacetone, CMV PCR, blood IEM screening, was negative and serum ferritin was mildly raised. Due to fulminant sepsis, uncorrected coagulopathy with multiorgan dysfunction, the baby expired after 1 month of hospital stay. Liver biopsy done posthumously because of deranged coagulation profile, suggestive of cholestasis with bridging fibrosis. Genetic work up was sent which revealed Galactosemia, variant c.562C>T, homozygous, location-exon 6.
Figure 1. Galactosemia with ascitis, peritoneal dialysis catheter in situ.
Case 2:
A 9 days old late preterm, newborn admitted with abdomen distension since birth. USG abdomen was suggestive of ascitis. Ascitic tap revealed yellowish white fluid with cell count 3200/cu mm, 92% lymphocyte, triglyceride level was 397 mg/dl which was suggestive of chylous ascitis. Started on TPN followed by MCT powder feeds and ocreotide infusion. Blood culture revealed growth of Kleibsella. Abdomen distension progressively increased, so ascitic fluid drain was done repeatedly with albumin cover which lead to peritonitis. Due to uncontrolled sepsis baby also received immunoglobulin .Sepsis gradually got settled with appropriate antibiotics and general condition improved. Lymphoscintigraphy was planned but ,could not be done.MRI abdomen done which revealed ascitis with no other significant abnormality. Exploratomy laparotomy was planned to look for any lymphatic vessel abnormality but was cancelled due to dense adhesions. Baby was discharged after 1.5 months of NICU stay on MCT powder feeds in a haemodynamically stable condition.
Case 3:
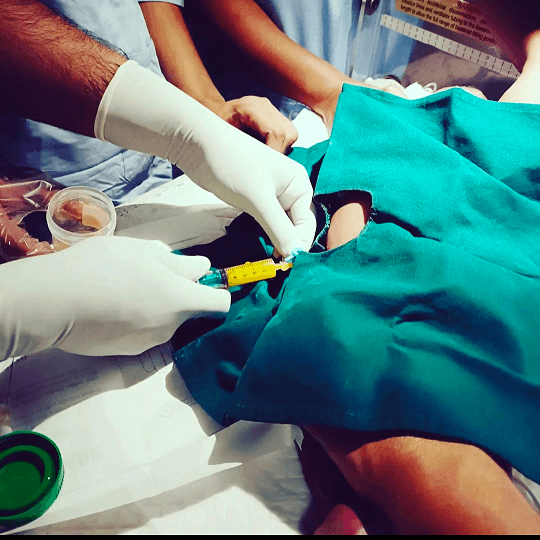
A term male baby presented with abdomen distension since birth. Ultrasound was suggestive of ascites. Ascitic fluid tap was done, appearance was milky with cell count 5500/cu mm and triglyceride was 1188 mg/dl which was suggestive of chylous ascites. Aggressive TPN support followed by ocreotide infusion and MCT powder feed was given. Baby was not having any symptomatic improvement. He was having persistent hypoalbuminemia inspite of albumin transfusion so received multiple albumin transfusion and IVIg also due to uncontrolled sepsis. Upper GI endoscopy was done which was suggestive of intestinal lymphangectasia. Gradually baby also developed chylous pleural effusion. The baby expired after 3 months of hospital stay.
Figure 2. Ascitic tap done in a chylous ascitis patient.
Case 4:
A 10 days old baby was admitted with abdomen distension with decreased urine output and dribbling of urine noticed since day 3 of life. USG abdomen was suggestive of bilateral gross hydronephrosis. Serum electrolytes and urea, creatinine was normal. MCUG was done which was suggestive of posterior urethral valve. PUV fulguration was done and overnight, baby developed abdomen distension and decreased urine output. USG whole abdomen was suggestive of ascites. In view of suspected urinary ascites, ascitic fluid creatinine was sent and it was raised 1.6 mg/dl while serum creatinine was 0.5 mg/dl. Peritoneal drainage and bilateral uterostomy was done on the next day. Post operatively baby developed kleibsella sepsis which was treated and discharged in a haemodynamically stable condition and advised for follow up.
Case 5:
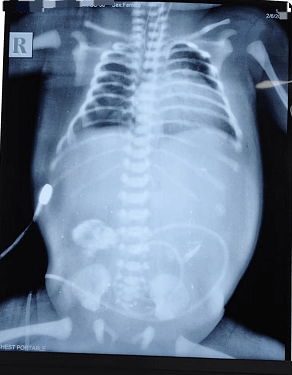
A 33 weeks female newborn was admitted on day 1 with respiratory distress after birth with abdomen distension. Chest and abdomen X-ray was done, suggestive of lower end esophageal obstruction, ascites and 3 irregular opaque shadows in abdomen. 2D echo was done, there was no pericardial effusion. USG abdomen suggestive of meconium pseudocyst with calcification and ascites. Ascitic tap was done which was suggestive of peritonitis. Ascitic fluid cell count was 1320/cu mm with neutrophilic predominance with protein 3 gm/dl. Laparotomy was done which revealed ileal perforation 4 cm proximal to the ileocaecal junction and dense adhesion, so ileostomy was done. Ascitic fluid culture sensitivity was negative but blood culture had grown MDR Kleibsella. Baby ultimately expired due to septicaemia.
Figure 3. Meconium peritonitisto.
| | | | Discussion | Though urinary ascites is the most commonly reported cause of ascites in newborn but out of above 5 cases, 2 of them had chylous ascites. Similar result was noted in a study done by Chaudhury etal3 which showed chylous ascites is the most common cause. About 50% of cases are caused due to malformation of lymphatic vessels and remaining may be caused due to external compression of the lymphatics, trauma, child abuse. Most of them has no etiology and is due to delay in maturation of the lacteals, called “leaky lymphatics”.4 It is diagnosed by lymphocyte-rich, milky peritoneal fluid with triglycerides >110 mgr/dl. The imaging study of choice is lymphoscintigraphy but it is mostly avoided because of technical difficulties in a sick neonate. This condition is often refractory to treatment and causes severe EUGR, immunodeficiency and sepsis because of the loss of proteins and lymphocytes. IVIg can be given due to loss of immunoglobulins and sepsis.5 Treatment is mostly conservative, requires TPN, ocreotide infusion and MCT feeds.6,7 Mouravas etal reported that if any definite lesion like a chylous cyst is visible in ultrasound and MRI, then exploratory laparotomy can be done.8
Galactosemia, though can have progressive hepatic failure but ascites is rare. Lone KS etal reported 16.7% of early infantile liver failure due to galactosemia.9 Patients with galactosemia present with hypoglycaemia, jaundice, failure to thrive, lethargy, feeding difficulty, vomiting, diarrhea, sepsis, cataract and also hepatomegaly, liver failure and renal tubular dysfunction in severe cases. Patients who cannot be properly managed die due to liver failure, kidney failure, or sepsis.10 Grama A etal reported a case of galactosemia with group B streptococcus infection and acute liver failure.11 Ascites in galactosemia is rarely reported in past and develops 2-5 weeks after birth with continued galactose.12 Renal failure in early infancy is a rare manifestation of galactosemia. Nesrin C etal reported a case of galactosemia which required peritoneal dialysis due to metabolic acidosis.13 Hepatorenal syndrome is defined as AKI in liver failure in absence of shock, nephrotoxic drugs, no proteinuria, microhematuria and normal kidney ultrasound.14 In our patient with galactosemia, bilateral kidneys are hyperechoic and also he had significant proteinuria along with excretion of bile salts, urobilongen and bilirubin in urine which might have caused cholemic nephropathy which is diagnosed by kidney biopsy and has poor outcome.15
Meconium peritonitis is sterile chemical peritonitis due to intrauterine bowel perforation and meconium excretion into the peritoneal cavity seen as classic eggshell calcifications on X-ray. Incidence is 1 in 35 000 and has high mortality.16 A. Lamrissi studied that clinical features of MP are non-specific and may be asymptomatic also. Antenatal diagnosis by obstetrical ultrasound can be done. On examination there is abdominal distension and an mass, commonly in the right lower quadrant. Meconium peritonitis after birth results in bacterial sepsis with results in poor prognosis. Meconium peritonitis may be due to meconium ileus, intestinal stenosis or atresia etc.17 Ruptured ileum is the most common pathology.18 Cystic fibrosis is associated with 8-40% cases.19 Chiba T et al described two cases of ileal artesia with perforation and fetal ascites due to meconium peritonitis.20 IV antibiotics, laparotomy, drainage, temporal enterostomy with delayed reconstruction of intestinal continuity is the management of choice.21
Neonatal urinary ascites is also a rare condition. It can be spontaneous or iatrogenic. It is a life-threatening condition as the peritoneal membrane "autodialyzes" the urine, leading to deranged electrolytes and kidney function test. Posterior urethral valve is the most common cause of spontaneous urinary ascites which occurs due to rupture of calyceal fornices or urinary bladder perforation.22 Yue He reported Neonatal Urinary Ascites due to Anterior Urethral Valve and Diverticulum in Preterm Newborn.23 USG is the 1st line of investigation in urinary ascites. MCUG is used to detect the site of leak in the urinary.24 Ascites Cr: serum Cr ratio of over 1 is diagnostic of urinary ascites.25 Management consists of catheter drainage or surgery to divert the urine from the peritoneal cavity.26 | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Chou YY, Huang HC etal. Isolated fetal and neonatal ascites: report of two cases. Acta Paediatr Taiwan. 2001 May-Jun;42(3):166-8. PMID: 11431863.
- Griscom NT, Colodny AH etal. Diagnostic aspects of neonatal ascites: report of 27 cases. AJR Am J Roentgenol. 1977 Jun;128(6):961-9. doi: 10.2214/ajr.128.6.961. PMID: 414563. [CrossRef]
- Chaudhuri etal. Neonatal Ascites- Experience from a Tertiary Care Centre.Journal of Medical Science and Clinical Research.2018.June;Vol 06,Issue 06,Page 197-201.
- Romańska-Kita J, Borszewska-Kornacka MK etal. Congenital chylous ascites. Pol J Radiol. 2011 Jul;76(3):58-61. PMID: 22802843; PMCID: PMC3389932.
- Sooklin L, Anand AJ etal. Management of large congenital chylous ascites in a preterm infant: fetal and neonatal interventions. BMJ Case Rep. 2020 Sep 2;13(9):e235849. doi: 10.1136/bcr-2020-235849. PMID: 32878831; PMCID: PMC7470640. [CrossRef]
- Caty MG, Hilfiker M etal. Successful treatment of congenital chylous ascites with a somatostatin analogue. Pediatr Surg Int. 1996 Jun;11(5-6):396-7. doi: 10.1007/BF00497824. Epub 2013 Sep 21. PMID: 24057727. [CrossRef]
- Purkait R, Saha A etal. Congenital chylous ascites treated successfully with MCT-Based formula and octreotide. J Indian Assoc Pediatr Surg. 2014 Jul;19(3):175-7. doi: 10.4103/0971-9261.136480. PMID: 25197199; PMCID: PMC4155638. [CrossRef]
- Mouravas V, Dede O, Hatziioannidis H etal. Diagnosis and management of congenital neonatal chylous ascites. Hippokratia. 2012 Apr;16(2):175-80. PMID: 23935276; PMCID: PMC3738422.
- Lone KS, Al Saleem B etal. Liver Failure Among Young Saudi Infants: Etiology, Clinical Presentation, and Outcome. J Pediatr Gastroenterol Nutr. 2020 Feb;70(2):e26-e32. doi: 10.1097/MPG.0000000000002554. PMID: 31978013. [CrossRef]
- Karadağ N, Okbay Güneş A etal. Acute liver failure in newborns. Turk Arch Pediatr. 2021 Feb 3;56(2):108-114. doi: 10.5152/TurkArchPediatr.2021.190205. PMID: 34286318; PMCID: PMC8269940. [CrossRef]
- Grama A, Blaga L, Nicolescu A etal. Novel Mutation in GALT Gene in Galactosemia Patient with Group B Streptococcus Meningitis and Acute Liver Failure. Medicina (Kaunas). 2019 Apr 4;55(4):91. doi: 10.3390/medicina55040091. PMID: 30987402; PMCID: PMC6524007. [CrossRef]
- Maşallah Baran , Kayı Eliaçık etal.Neonatal Ascites and Liver Failure: A Case of Galactosemia.2012. Smyrna Tıp Dergisi.34-36.
- Nesrin C, Nihat D etal, An Unusual Presentation of Galactosemia in the Newborn: Liver Failure and Hyperammonemia,Journal of Contraceptive Studies,2016, Vol.1 No.3:16.
- Acevedo JG, Cramp ME. Hepatorenal syndrome: Update on diagnosis and therapy. World J Hepatol. 2017 Feb 28;9(6):293-299. doi: 10.4254/wjh.v9.i6.293. PMID: 28293378; PMCID: PMC5332418. [CrossRef]
- Sood V, Lal BB etal. Cholemic or Bile Cast Nephropathy in a Child with Liver Failure. J Clin Exp Hepatol. 2017 Dec;7(4):373-375. doi: 10.1016/j.jceh.2017.05.006. Epub 2017 May 15. PMID: 29234203; PMCID: PMC5715444. [CrossRef]
- Sharma D, Murki S, Pratap T. Meconium peritonitis: an interesting entity. BMJ Case Rep. 2014 May 5;2014:bcr2014203536. doi: 10.1136/bcr-2014-203536. PMID: 24798361; PMCID: PMC4025370. [CrossRef]
- Lamrissi A, Madri FE, Wajih O, Mourabbih M, Jalal M, Bouhya S. Mecomium peritonitis: A case report. Int J Surg Case Rep. 2022 Sep;98:107476. doi: 10.1016/j.ijscr.2022.107476. Epub 2022 Aug 4. PMID: 35987026; PMCID: PMC9404345. [CrossRef]
- Gudi SN, Bhanuprakash MR, Suneetha V, Prasanna N. Meconium pseudocyst and ileal atresia secondary to intrauterine intussusception. J Obstet Gynaecol India. 2011 Oct;61(5):562-4. doi: 10.1007/s13224-011-0089-5. Epub 2011 Oct 27. PMID: 23024531; PMCID: PMC3257327. [CrossRef]
- Chiba T, Ohi etal. Ileal atresia with perforation in siblings. Eur J Pediatr Surg. 1991 Feb;1(1):51-3. doi: 10.1055/s-2008-1042460. PMID: 2031917. [CrossRef]
- Sathe M, Houwen R. Meconium ileus in Cystic Fibrosis. J Cyst Fibros. 2017 Nov;16 Suppl 2:S32-S39. doi: 10.1016/j.jcf.2017.06.007. PMID: 28986020. [CrossRef]
- Uchida K, Koike Y, Matsushita K etal. Meconium peritonitis: Prenatal diagnosis of a rare entity and postnatal management. Intractable Rare Dis Res. 2015 May;4(2):93-7. doi: 10.5582/irdr.2015.01011. PMID: 25984428; PMCID: PMC4428193. [CrossRef]
- Gupta P, Gupta AK, Aggarwala S. Urinary Ascites Secondary to Bladder Perforation in a Neonate with Posterior Urethral Valves. Oman Med J. 2013 Jul;28(4):e051. doi: 10.5001/omj.2013.85. PMID: 31435473; PMCID: PMC6667814. [CrossRef]
- He Y, Lin SB, Li W, Sun Y etal. Case Report: Neonatal Urinary Ascites Without Hydronephrosis: A Rare Case of Anterior Urethral Valve and Diverticulum in Preterm Newborn. Front Pediatr. 2022 Jun 30;10:920817. doi: 10.3389/fped.2022.920817. PMID: 35844749; PMCID: PMC9280888. [CrossRef]
- Syed M. Qurram, C. V. S. Lakshmi etal. International Journal of Contemporary Pediatrics. 2021 Jun;8(6):1125-1127. [CrossRef]
- Zhuang TZ, Akhnoukh SB etal. Urinary Ascites: An Imitator of Portal Hypertension-Related Ascites. Cureus. 2022 Sep 25;14(9):e29581. doi: 10.7759/cureus.29581. PMID: 36321002; PMCID: PMC9596943. [CrossRef]
- Solarin A, Gajjar P. Neonatal urinary ascites: a report of three cases. Case Rep Nephrol. 2015;2015:942501. doi: 10.1155/2015/942501. Epub 2015 Apr 14. PMID: 25954559; PMCID: PMC4411504. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2025.72
|
| Cite this article as: | | Ghosh S, Uttam K G, Khemka P, Islam R, Kabir S. Neonatal ascites - a case series. Pediatr Oncall J. 2025;22: 193-195. doi: 10.7199/ped.oncall.2025.72 |
|