Karuna Thapar, Gaurav Dhawan, Sandeep Aggarwal, Naresh Jindal.
Department of Pediatrics, Government Medical College, Amritsar.
ADDRESS FOR CORRESPONDENCE
Karuna Thapar, Hno. 9-A, Krishna Square, Near Shivala Mandir, Amritsar-143001.
Email: kthapar2000@yahoo.com | REDUNDANT DUE TO DUPLICATE PUBLICATION
A one & half year old male child presented with gradually increasing size of second & third toe of right foot since birth. (Figure 1).
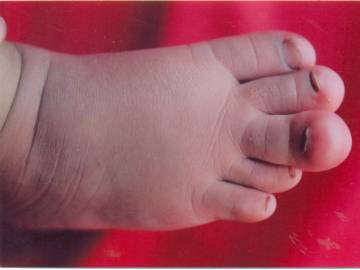
There was no family history of hypertrophy of limbs; no history of pigmentation and seizures. On local examination swelling was soft, non tender, non pulsatile, non fluctuating with no change in color or rise in temperature, transillumination test was negative. General physical examination and systemic examination were within normal limits. He was evaluated by X-ray foot that revealed hypertrophy of soft tissues & bones (distal phalanges) of second & third digits. On ultrasonography there was hypertrophy of fibroadipose tissue of right second & third toe. The soft tissue distribution was typically more towards the distal end of the involved toes on the dorsal & volar aspects. There were no osteolytic or sclerotic lesions in the involved bones. Color Doppler showed no evidence of any increased flow in the above region to suggest any vascular malformation. MRI could not be performed due to cost factor. This clinical history, together with the radiographic & ultrasonographic findings suggested the diagnosis of Macrodystrophia lipomatosa.
Macrodystrophia lipomatosa (ML) is a rare cause of focal gigantism which was first described in 1925 by Feriz (1). It has also been called as partial acromegaly, macrosomy, elephantiasis, megalodactly, dactylomegaly, macrodactyly and limited gigantism. Although the certain etiology of the disease has not been known yet, lipomatous degeneration, fetal circulation abnormality, and damage of extremity bud in intrauterine life are some of the proposed hypothesis. It is now believed to be a part of generalized hamartomatous disorder known as Proteus syndrome (2). Deformity is realized just after delivery. This condition is found in both the upper and lower extremities. The condition may affect more than one finger; even it may involve the whole extremity. The most commonly involved parts are the second and third fingers of the upper or lower extremity. Bilateral involvement is very rare. Most cases involve the middle and index fingers, corresponding to the territory supplied by the branches of the median nerve (1, 3). The differential diagnosis includes neurofibromatosis, proteus syndrome Klippel-Trenaunay-Weber syndrome, lymphangiomatosis, hemangiomatosis, and fibrolipomatous hamartoma of the nerve. Imaging modalities like X-ray, Ultrasonography, Magnetic Resonance Imaging (MRI) or Computed Tomography (CT) can be used to evaluate the affected parts. On conventional X-Ray images macrodactyly and soft tissue overgrowth are visible and are most marked along the volar aspect of the digit and at its distal end. This overgrowth can produce dorsal deviation of affected parts (4). Radiolucent areas within increased soft tissue shadows due to adipose tissue are occasionally seen (5). The phalanges are elongated, broad, and the distal ends are splayed and can have a "mushroom" shape (6). Slanting of the articular surfaces can occur and this leads to secondary degenerative joint disease, manifesting as subchondral cyst and osteophyte formation (7). The etiology of the development of the secondary degenerative change, which occurs in adults, is unclear. Excessive growth of the bone within the area innervated by nerve and fat tissue proliferation within muscle fibers are the characteristic findings detected by CT. MRI is also a useful imaging modality to aid diagnosis.
Abnormal growth of the involved finger ceases in puberty. Surgical intervention is usually carried out due to cosmetic reasons but proper information about the nature of the disease should be given to the patient before performing surgical intervention. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Kelikian H. Congenital deformities of the hand and forearm. Philadelphia: Saunders 1974; 610-635.
- Broadwater BK, Major NM, Goldner RD, LayField. Macrodystrophia lipomatosa with associated fibrolipomatous hamartoma of the median nerve. Pediatric surgery 2000; 16: 216-285. [CrossRef] [PubMed]
- Barsky AJ. Macrodactyly. J Bone Joint Surg 1967; 49(A): 1255-1265.
- Baruchin AM, Herold ZH, Shmueli G, Lupo L. Macrodystrophia lipomatosa of the foot. J Pediatr Surg 1988; 23(2): 192-194. [CrossRef]
- D'Costa H, Hunter JD, O'Sullivan G, O'Keefe D, Jenkins JP, Hughes PM. Magnetic resonance imaging in macromelia and macrodactyly. Br J Radiol 1996; 69(822): 502-507. [CrossRef] [PubMed]
- Gupta SK, Sharma DP, Sharma SU, Sood B, Gupta S. Macrodystrophia lipomatosa: radiographic observations. Br J Radiol 1992; 65(777): 769-773. [CrossRef] [PubMed]
- Levine C. The imaging of body asymmetry and hemihypertrophy. Crit Rev Diagn Imaging 1990; 31(1): l-80.
|
| Cite this article as: | | Thapar K, Dhawan G, Aggarwal S, Jindal N. Macrodystrophia Lipomatosa-A Case Report. Pediatr Oncall J. 2007;4: 50. |
|