Rajesh Kulkarni, Ashok D Rathod.
Department of Pediatrics, JJ Hospital, Mumbai.
ADDRESS FOR CORRESPONDENCE
Dr Rajesh Kulkarni, Lecturer in Pediatrics, CWC Building, Grant Medical College and JJ Hospital JJ Hospital Campus, Byculla, Mumbai 400008.
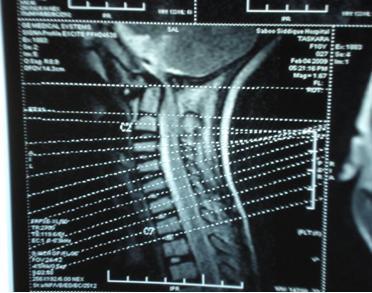
Email: docrajesh75@yahoo.com | A 10 year old female child was brought with history of weakness of left lower limb since 11 months, right lower limb since 10 ½ months and left upper limb since 8 months. Child was apparently alright one year back when she started having recurrent falls while walking and running. This was followed by weakness in left lower limb and, 15 days later, she started having weakness of right lower limb. The weakness gradually progressed over a period of 3 months such that she initially had difficulty in walking, later she could walk only with support and also could not stand up from sitting position. Since last 3 months patient is bed ridden & sits only with support. There was a history of weakness of proximal muscles in left upper limb since 8 months. Child was able to lift right hand above head but with difficulty. There was no history suggestive of cortical, cranial nerve, bladder or sensory involvement. On examination of motor system there was asymmetrical proximal muscle weakness (left more than right) in lower limbs as well as upper limbs with brisk deep tendon reflexes. Sensory system examination was normal .There was no abnormality on examination of the spine. MRI Cervical Spine and 3 D CT cervical spine revealed cranio vertebral junction anomaly with os - Odontoidium, atlanto- axial dislocation and congenital fusion of C2 and C3 vertebral bodies with cord compression by posterior superior portion of C2 with cord edema/myelomalacia at C1/C2 level and severe secondary canal stenosis at C2/C3 levels. (Figure 1) Patient was given high dose steroid for spinal cord edema. Strict immobilization of spine with hard neck collar was done. The patient has been referred for traction & operative stabilization by wiring and screw fixation.
Figure 1: MRI spine showing os - Odontoidium, atlanto- axial dislocation and congenital fusion of C2 and C3 vertebral bodies with cord compression by posterior superior portion of C2.
In 1886, Giacomini coined the term os odontoideum .This entity is clinically important because the mobile or insufficient dens renders the transverse atlantal ligament (TAL) ineffective at restraining atlantoaxial motion. Translation of the atlas on the axis may lead to impingement of the upper cervical cord or vertebral artery. Os odontoideum is rare, but the exact prevalence and incidence are unknown. Many cases are either incidentally detected or are diagnosed when patients become symptomatic. The age at diagnosis varies significantly from the first to the sixth decades of life. With increased awareness, however, os odontoideum has been diagnosed in younger patients. While the etiology remains controversial an increased frequency of os odontoideum has been reported in patients with multiple epiphyseal dysplasia and Down's syndrome .(1-3) Some authors speculate that os odontoideum represents a previous fracture of the odontoid synchondrosis before its closure at age 5-6 years. These authors describe os odontoideum in patients with previously normal cervical radiographs. For example, Schuler et al elegantly described the evolution of an os odontoideum following trauma in a child .(4)
In patients with os odontoideum, management principles are clinical and radiologic surveillance in asymptomatic patients, high dose steroids for spinal cord edema, strict immobilization of spine by hard neck collar, traction and operative stabilization in the form of wiring and screw fixation if there is spinal instability, neurologic involvement or intractable pain. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Morgan MK, Onofrio BM, Bender CE. Familial os odontoideum. Case report. J Neurosurg. 1989; 70: 636-639. [CrossRef] [PubMed]
- Stevens JM, Chong WK, Barber C, Kendall BE, Crockard HA. A new appraisal of abnormalities of the odontoid process associated with atlanto-axial subluxation and neurological disability. Brain. 1994; 117 ( Pt 1): 133-148. [CrossRef] [PubMed]
- Verska JM, Anderson PA. Os odontoideum. A case report of one identical twin. Spine. 1997; 22: 706-709. [CrossRef]
- Schuler TC, Kurz L, Thompson DE, Zemenick G, Hensinger RN, Herkowitz HN. Natural history of os odontoideum. J Pediatr Orthop. 1991; 11: 222-225. [CrossRef] [PubMed]
|
| Cite this article as: | | Kulkarni R, Rathod A D. Os odontoideum. Pediatr Oncall J. 2010;7: 52. |
|