|
Bony Swellings
Rahul Sinha1, Vandana Negi2, S S Dalal3.
1Department of Pediatrics, 167 Military Hospital, Pathankot,
2Army Hospital, New Delhi,
3Command Hospital Air Force, Bangalore, India.
ADDRESS FOR CORRESPONDENCE
Dr Rahul Sinha, 167 Military Hospital, Pathankot, Punjab India.
Email: drrahul_2000@yahoo.com
|

|
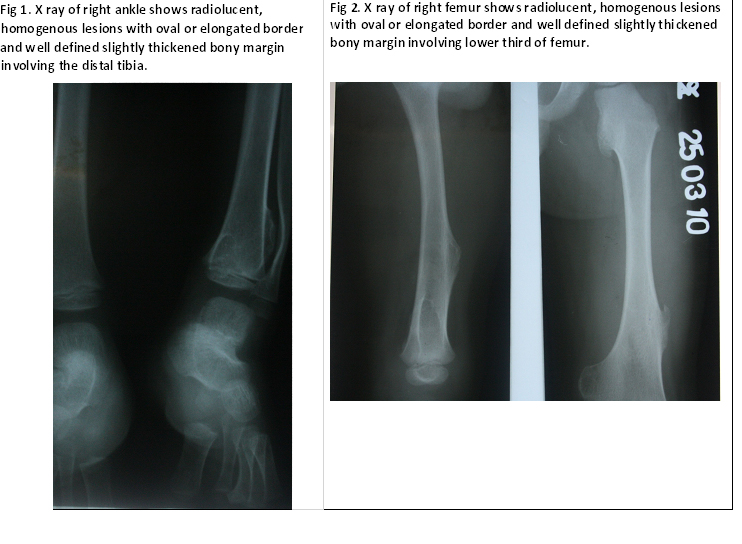
What is the diagnosis?
Ollier’s disease. It is a rare nonhereditary sporadic disorder where intraosseous benign cartilaginous tumors develop close to growth plate cartilage. Prevalence is estimated at around 1 in 100,000. {1} The disease consists of multiple enchondromas which usually develop in childhood. On radiographs, streaks of low density are seen projecting through the diaphyses into the epiphyses of the long bones, due to ectopic cartilage deposits. With age, the cartilage may calcify in the typical snowflake pattern. The affected extremity is shortened {asymmetric dwarfism} and sometimes bowed due to epiphyseal fusion anomalies. Differential diagnoses include Maffucci syndrome which is characterized by multiple enchondromatosis as well as multiple soft tissue cavernous hemangiomas, and less commonly lymphangiomas which was not seen in our patient. {2} Both Maffucci syndrome and Ollier`s disease are associated with an increased incidence of juvenile granulosa cell tumor of the ovary. {3} Patients with Maffucci syndrome also have an increased incidence of malignancies other than musculoskeletal malignancies, including gliomas, gastrointestinal adenocarcinoma, pancreatic carcinomas and ovarian tumor. {3,4} Another differential diagnosis to be considered is metachondromatosis which is a hereditary autosomal dominant transmitted condition consisting of multiple enchondromas and osteochondromas. In this syndrome, the multiple exostoses characteristically occur in the digits and long bones, point towards the joints and frequently regress spontaneously. {5} The most important criterion to distinguish enchondromas from osteochondromas is the localization of bone lesions: osteochondromas are located at the bone surface and enchondromas are located in the center of bones, thus allowing radiographic distinction.
Persons with Ollier disease are prone to breaking bones and normally have swollen, aching limbs. There is no medical treatment for enchondromatosis. Surgical intervention is indicated in case of complications {pathological fractures, growth defect, malignant transformation}.
E-published: June 2012 Vol 9 Issue 6 Art # 38 |
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
|
- Khoo RN, Peh WC, Guglielmi G. Clinics in diagnostic imaging (124). Multiple enchondromatosis in Ollier disease. Singapore Med J 2008;49: 841-845 [PubMed]
- Zwenneke Flach H, Ginai AZ, Wolter Oosterhuis J. Best cases from the AFIP. Maffucci syndrome: radiologic and pathologic findings. Armed Forces Institutes of Pathology. Radiographics. 2001; 21: 1311-1316 [CrossRef] [PubMed]
- Tamimi HK, Bolen JW. Enchondromatosis (Ollier's disease) and ovarian juvenile granulosa cell tumor. Cancer. 1984; 53: 1605-1608. [CrossRef]
- Mahafza WS. Multiple enchondromatosis Ollier's disease with two primary brain tumors. Saudi Med J. 2004; 25: 1261-1263 [PubMed]
- Schwarz W, Hardes J, Schulte M. Multiple enchondromatosis: Ollier's disease. Unfallchirurg. 2002; 105: 1139-1142 [CrossRef] [PubMed]
|
|
DOI: https://doi.org/10.7199/ped.oncall.2012.38 |
| |
Cite this article as:
Sinha R, Negi V, Dalal S S. Bony Swellings (Ollier`s disease). Pediatr Oncall J. 2012;9: 55. doi: 10.7199/ped.oncall.2012.38
|