Shweta Anand, Amit Agrawal.
Department of Pediatrics, Gandhi Medical College and Kamla Nehru Hospital, Bhopal, India.
ADDRESS FOR CORRESPONDENCE
Dr Amit Agrawal, 28, Ravidas Nagar, Near Nizamuddin Colony, Indrapuri, Bhopal, MP, India.
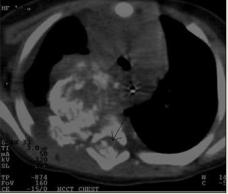
Email: agrawaldramit@yahoo.co.in | | Keywords | | Chylothorax, Neuroblastoma, Mediastinal Mass, Respiratory Distress | | | A four months old male baby was brought to emergency with history of cough and breathlessness for past seven days. On examination child was afebrile, with heart rate - 140/min, respiratory rate - 50/min and blood pressure 70/40 mmHg. SpO2 was 70% on room air which increased to 92% with 100% oxygen. Respiratory examination showed marked intercostal and subcostal retractions with decreased air entry on the right side of chest. Rest of the systemic examination was within normal limits. X-ray chest showed evidence of pleural effusion with a well defined large heterogeneous lobulated mass containing coarse calcifications in right thoracic paravertebral region. (Fig. 1) Provisional diagnosis of pleural effusion was made and supportive therapy was started with oxygen supplementation, intravenous fluids and parenteral antibiotics. To relieve respiratory distress, intercostal tube drainage was performed, through which milky white fluid was drained which was sent for analysis. On analysis, specific gravity of pleural fluid was 1.012; leukocyte count was 5000/µL with 90% lymphocyte, while the triglyceride and cholesterol content were 220 and 50 mg/dl respectively. Lipoprotein electrophoresis of fluid showed a chylomicron band. All these investigations were conclusive of chylothorax. Contrast enhanced CT chest revealed a large (5.3x5.8x7.5 cm) well defined heterogeneous contrast enhancing mass containing coarse calcification in paraspinal region of upper half of thorax, extending into spinal canal (T2-T5) and displacing the mediastinal structures (Fig. 2) suggestive of neoplastic etiology (most probably neuroblastoma). CT abdomen and head were normal. CT guided fine needle aspiration cytology (FNAC) showed few sheets of small monomorphic round cells with hyperchromatic nuclei having evenly distributed chromatin without prominent nucleoli associated with fibrillary appearing process. At places small calcific deposit were seen with scattered inflammatory cells (lymphocytic predominance). Cytology was suggestive of round cell tumor most probably neuroblastoma. The 24 hour urinary Vanillyl mandelic acid was elevated (75µg/dl) confirming the diagnosis. Patient was put on parenteral nutrition and diet containing high protein and medium chain triglyceride with low fat. Fresh frozen plasma was transfused intermittently. As patient was not responding to conservative management, octreotide was started on day seven initially at a dose 0.5mcg/kg/hr and subsequently increased to 5mcg/kg/hr with daily increment of 1mcg/kg/hr. After ten days of therapy, the octreotide was discontinued in view of the satisfactory response. No side effect was noted during or after octreotide therapy. Amount of fluid from the drain gradually reduced, so chest tube was removed. After stabilization patient was referred to oncologist for chemotherapy but was lost to follow up.
Fig. 1: X- ray chest showing coarse calcifications in right thoracic paravertebral region.

Fig. 2: Contrast enhanced CT chest showing coarse calcification in paraspinal region displacing the mediastinal structure and extension into spinal canal (Arrow)
Thoracic masses arising from the mediastinum pose a diagnostic dilemma in the pediatric age group. Neuroblastoma is the most common malignant cause of mediastinal mass in children under the age of two years. (1) Neuroblastoma accounts for 6-10% of childhood cancers. (2,3) Neuroblastoma can arise from any neural crest element of sympathetic nervous system. This site of origin along with metastasis (if any) at the time of presentation and metabolically active by-product determines clinical presentation. The presenting features of neuroblastoma vary depending on its size, location and extent of tumor spread. Mc Latchie et al found that out of seven cases of primary thoracic neuroblastoma, two presented with respiratory symptoms. (4) One rare presentation of thoracic neuroblastoma is chylothorax. Neuroblastoma produces chylothorax due to either extrinsic compression or infiltration of the thoracic duct, which causes increase in intraductal pressure. This increased pressure promotes the formation of dilated collateral channels that eventually drain into pleural space leading to chylothorax. (5)
Very scanty literature is available regarding the incidence of chylothorax in children; however, it is predominantly seen as a complication following cardiothoracic surgery and occasionally in newborns. Lymphomas are the most common type of tumour associated with chylothorax (60 - 70% of cases) however; any mediastinal tumour (e.g. teratoma and neuroblastoma) has the potential to cause chylothorax in children. (5) A milky or turbid appearance of the fluid may also be seen with an empyema or when there is a chronic pleural effusion with high cholesterol content but no triglycerides or chylomicrons (pseudochylothorax). Therefore, chylothorax must be diagnosed by biochemical analysis of the fluid. The key finding is the presence of chylomicrons, which can be demonstrated better after staining with Sudan III. (6). On the basis of review of literature, conservative management should be treatment of choice while surgical treatment should be reserved for the cases in which clinical improvement does not occur within two weeks and should consist of thoracic duct ligation. (7) In our case, patient responded to conservative management (dietary, intercostal drainage and octreotide therapy). | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Saenz NC, Schnitzer JJ, Eraklis AE, Hendren WH, Grier HE, Macklis RM, et al. Posterior mediastinal mass. J Pediatr Sur 1993; 28: 172-176. [CrossRef]
- Park JR, Eggert A, Caron H. Neuroblastoma: biology, prognosis, and treatment. Pediatr Clin North Am 2008; 55: 97-120. [CrossRef]
- Stiller CA, Parkin DM. International variations in the incidence of neuroblastoma. Int J Cancer. 1992; 52: 538-543. [CrossRef]
- McLatchie GR, Young DG. Presenting features of thoracic neuroblastoma. Arch Dis Child 1980; 55: 958-962. [CrossRef]
- Soto-Martinez M, Massie J. Chylothorax: Diagnosis and Management in Children. Paediatr Respir Rev. 2009; 10: 199-207. [CrossRef]
- Staats BA, Ellefson RD, Budahn LL, Dines DE, Prakash UB, Offord K. The lipoprotein profile of chylous and nonchylous pleural effusions. Mayo Clin Proc 1980; 55: 700-704. [PubMed]
- Beghetti M, La Scala G, Belli D, Bugmann P, Kalangos A, Le Coultre C. Etiology and management of pediatric chylothorax. J Pediatr 2000; 136: 653-658. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2012.64
|
| Cite this article as: | | Anand S, Agrawal A. Neuroblastoma Presenting as Chylothorax. Pediatr Oncall J. 2012;9: 107-108. doi: 10.7199/ped.oncall.2012.64 |
|