R Sujetha1, T Palanivelraja2, K S Kumaravel3, S Gobinathan4, P Sampathkumar3.
1Junior Resident, Department of Pediatrics, Govt. Mohan Kumaramangalam Medical College, Salem,
2Assistant Professor, Department of Pediatrics, Govt. Mohan Kumaramangalam Medical College, Salem,
3Professor, Department of Pediatrics, Govt. Mohan Kumaramangalam Medical College, Salem,
4Associate Professor, Department of Pediatrics, Govt. Mohan Kumaramangalam Medical College, Salem.
ADDRESS FOR CORRESPONDENCE
Dr. K.S.Kumaravel, M.D (Paediatrics), 191A, Shankar Nagar, Salem, Tamil Nadu, India. PIN: 636 007.
Email: kumaravelks@rediffmail.com | | Keywords | | constriction ring, dysplasia, oligohydramnios | | | A 23-year-old second gravida mother with 33 weeks of gestation was referred to our hospital in active labour. She had a spontaneous abortion 2 years back and she was a known case of situs inversus totalis. She was diagnosed to have hypothyroidism and was on levothyroxine for the past 2 years. She had a non consanguineous marriage. There was no other significant ante natal history. Serial ultra sonograms were done ante-nataly for the mother. Fusion of amnion was observed only at 20 weeks of gestation. A constriction band in the right leg and resultant edema in the right foot was observed sonographically at 28 weeks of gestation (Fig: 1). She was taken for emergency cesarean section (Indication: Breech presentation/Premature Rupture of membranes/Oligohydramnios) and a male baby weighing 1500 grams was delivered. During the delivery, the right leg of the baby just above the level of ankle along with the right foot which was attached with a very narrow pedicle, got separated (Fig: 2). The separated right leg and foot was edematous and focal areas of necrosis were seen. There were no other congenital anomalies like cleft palate/lip, amputation of fingers or syndactyly was noted. Post natal screening echocardiogram, cranial ultra sonogram and abdominal ultra sonogram were normal. The baby was given regular neonatal care and was discharged on 12th day.
Figure 1. Antenatal Ultrasonogram done at 28 weeks of gestation showing the constriction ring.
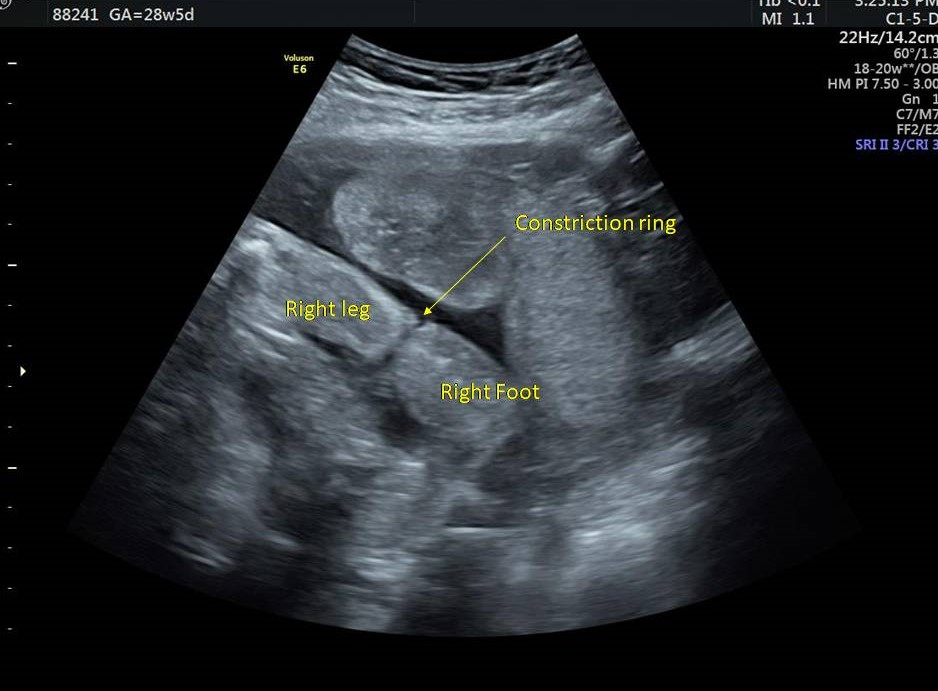
Figure 2. Neonate with separated Right foot.

Amniotic band syndrome (ABS) or Streeter’s dysplasia is a very rare congenital disorder with an incidence ranging from 1 in 1,000 to 1 in 15,000 live births.1 There is no gender preponderance and it is not inherited. The etiology is largely unknown. But it has been postulated that the rupture of amnion early in the pregnancy leads to multiple loose strands of amniotic bands which causes entanglement of fetal body parts and results in disruption, deformation or malformation.2 The spectrum of anomalies in ABS ranges from simple Streeter band to multiple severe cranio-facial anomalies.3 The spectrum includes clubfoot, facial clefting, choanal atresia, microphthalmia, syndactyly, lymphedema, phalangeal hypoplasia, limb shortening, pseudoarthrosis, peripheral nerve palsy, dystrophic nails, anencephaly, anterior abdominal wall defects, gastroschisis, bladder exstrophy, imperforate anus, omphalocele, cleft lip/palate and amputation of fingers/toes or hands or legs.4 Patterson et al in 1961 proposed diagnostic criteria for congenital ring constrictions, in which one or more of the following must be present to confirm the diagnosis – 1. Simple ring constrictions, 2. Ring constrictions associated with deformity of the distal body part with or without lymphedema, 3. Ring constrictions associated with fusion of distal body parts like syndactyly and 4. Intrauterine amputation of body parts.5
ABS can be diagnosed antenataly by 2 dimensional ultra sonogram at the end of the first or beginning of the second trimester. Three dimensional ultra sonogram in rendering mode, along with reconstruction of fetal surface, performed in the third trimester of pregnancy gives a better understanding about the constrictions and will help in the counseling of the families.6 The prognosis and treatment of ABS depends on the extent of the ring constriction and the body part involved. The prognosis is very good with simple constriction rings which can be treated with the release of the constriction ring. The children with auto amputation usually require reconstructive surgery or prosthesis.7 | | | | Acknowledgement | | The authors would like to acknowledge Dr.R.Subramanian, Consultant Sonologist, Sreenivas Ultrasound Scan Centre, Salem for his valuable contribution of sonographic images. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Kalousek DK, Bamforth S. Amnion rupture sequence in previable fetuses. Am J Med Genet. 1988 Sep;31(1):63-73. [CrossRef] [PubMed]
- Seeds JW, Cefalo RC, Herbert WN. Amniotic band syndrome. Am J Obstet Gynecol. 1982 Oct 01;144(3):243-8. [CrossRef]
- Srevatsa K, Gosavi M, Ranjit P, Joshi KM. Amniotic band syndrome: A case report and review of literature. J Sci Soc 2018;45:40-2. [CrossRef]
- The Journal of Foot and Ankle Surgery 1998;37:325-33. [CrossRef]
- Patterson TJ. Congenital ring‑constrictions. Br J Plast Surg 1961;14:1‑31. [CrossRef]
- Nardozza LM, Araujo Júnior E, Caetano AC, Moron AF. prenatal diagnosis of amniotic band syndrome in the third trimester of pregnancy using 3D ultrasound. J Clin Imaging Sci. 2012;2:22. [CrossRef] [PubMed] [PMC free article]
- Ashish M, Poonam M. Amniotic Band Syndrome. Pediatr Oncall J. 2012;9: 17-18. doi: 10.7199/ped.oncall.2012.8. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2022.49
|
| Cite this article as: | | Sujetha R, Palanivelraja T, Kumaravel K S, Gobinathan S, Sampathkumar P. Amniotic band syndrome: A case report and review of literature. Pediatr Oncall J. 2022;19: 134-135. doi: 10.7199/ped.oncall.2022.49 |
|