Inês Rosinha1, Helena Rios1, Joana Pinto2, Filipa Rodrigues1,3, José G. Soares4.
1Department of Pediatrics, Centro Hospitalar do Baixo Vouga, Aveiro, Portugal,
2Imaging Department and Neuroradiology Unit, Centro Hospitalar e Universitário de Coimbra, Portugal,
3Neurodevelopment Child Unit, Pediatrics Department, Centro Hospitalar do Baixo Vouga, Aveiro, Portugal,
4Department of Neurosurgery, Hospital Pediátrico, Centro Hospitalar e Universitário de Coimbra, Portugal.
ADDRESS FOR CORRESPONDENCE
Inês Mendonça de Oliveira Rosinha, Rua Fonte dos Amores nº 41, Avenal – Ul; 3720-584 – Oliveira de Azeméis, Portugal.
Email: inesmendrosinha@gmail.com | | Abstract | | Arachnoid cysts are benign congenital extra-axial malformations filled with cerebrospinal fluid, but not communicating with the ventricular system. Most are asymptomatic, usually found incidentally in neuroimaging studies. A two-year-old boy was referred for intermittent frontal headache that arose after falling from his own height the day before, with phonophobia, photophobia and triggered by exertion/defecation, and associated with a single postprandial vomiting. There were no visual complaints and no focal deficits on neurological examination. Neuroimaging studies revealed a left frontotemporal cystic lesion of 82x52x77mm, compressing insula and adjacent structures, and a bilateral subdural hygroma of probable posttraumatic etiology. He remained in hospital surveillance, maintaining hemodynamic stability and progressive clinical improvement, thereupon he was discharged and forwarded to Neurosurgery Consultation. Despite conventional neurosurgical treatment recommendation, newer reports suggest a promising role for the conservative approach, even in voluminous symptomatic lesions. This clinical case comes to corroborate the most recent evidence. | | | | Keywords | | Arachnoid cysts, subdural hygroma, middle temporal fossa, cerebrospinal fluid, neuroimaging studies, conservative/surgical treatment. | | | | Introduction | Primary arachnoid cysts (AC) are benign congenital well-circumscribed extra-axial malformations, filled with cerebrospinal fluid (CSF) and delimited by arachnoid membrane, which usually do not communicate with the ventricular system.1,2,3,4,5 Despite being the most common intracranial cysts, they are relatively rare, representing 1% of intracranial space-occupying lesions, with a prevalence of 1-3% in pediatric age.1,3,5 There seems to be a male-to-female preponderance of 2-5:1 and the left hemisphere is more often affected, both with no acceptable scientific explanation so far.1,5
AC are nearly always single and sporadic, mostly detected in the first two decades of life.2 Most of these simple cystic lesions of unknown etiology represent incidental findings on neuroimaging studies.2,5,6 Although these lesions can occur throughout the neuroaxis, more than half are found in the middle temporal fossa (MTF)/sylvian fissure.1,5 Other possible locations include the posterior fossa, suprasellar region and intraventricularly.1,5
Interestingly, many AC are detected during perinatal surveillance and long-term follow-up has revealed that some are quiescent throughout life; some may remain asymptomatic for many years before demonstrating signs and others may even disappear.1,2,6 With the greater worldwide availability of neuroimaging, more intracranial AC are being found in all age groups, but mostly in children (75%).2,3
The vast majority of AC are asymptomatic (93.2%), but occasionally AC may produce symptoms (6.8%) due to expansion or rupture, originating subdural hygroma (SH) or bleeding.1,5,7,8 Manifestations also depend on AC’s size and location, being headache the most common presenting symptom.2,5,8 Other possible symptoms are due to increased intracranial pressure, hydrocephalus or local mass effect.1,2,5 Hemorrhage is rare in the pediatric population (0.3-6%), trauma and larger cyst size being the main underlying risk factors.1,7
The overwhelming majority of lesions do not change in size relatively to the initial diagnosis and only rarely expand in the pediatric population, expansion primarily found under four years of age.1,5
| | | | Case Report | A two-year-old boy, with no personal/family history of note was brought to the emergency room due to headache that arose after falling from his own height the day before. The headache was intermittent, limited to the frontal region, with phonophobia and photophobia and was triggered by exertion (running) and defecation. A single postprandial vomiting was recorded. There were no visual complaints. On physical examination there were no traumatic injuries, the patient was conscious, with normal vital signs and there were no focal deficits in the neurological examination. Due to the headache’s persistence, he underwent on computed tomography (CT) head scan, which revealed a left frontotemporal cystic lesion with 27 x 54mm, with slight right deviation from the midline structures. Brain magnetic resonance imaging (MRI) confirmed a left temporal AC 82 x 52 x 77mm filling the temporal fossa and compressing insula and adjacent structures, with subfalcine herniation of 5 mm. It was also visualized a bilateral frontal SH of greater thickness on the left (4mm) of probable posttraumatic etiology, extending to the interhemispheric cleft. During the in-hospital surveillance he remained hemodynamically stable with progressive improvement in the headache. He was discharged with a recommendation for avoidance of high-impact physical activity. He is still regularly following up for neurosurgery consultation for clinical and radiological evaluation. During follow-up, the patient’s family reported some paroxysmal episodes of eye blinking usually lasting only a couple of seconds. Neurological examination was normal. A video-electroencephalogram was also performed and showed no abnormalities. There were no other complications and these paroxysms disappeared with time, as well as the headache. Subsequent brain-MRI revealed a progressive decrease in AC dimensions. On Figure 1, 7 months’ neuroimaging shows almost total resorption of the left hemispheric collection. Currently, he is 4 years old and is asymptomatic, without any restriction of physical activity, and there are no concerns about his neurodevelopment.
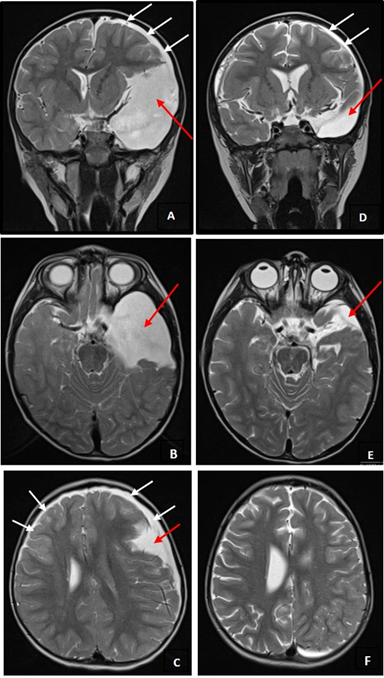
Figure 1. Brain-MRI T2-sequence images. A, B, C - Two days after head trauma: large left anterior temporal CA (evidenced by red arrows), conditioning right deviation of midline structures and left HS (evidenced by white arrows). D, E, F - Seventh month control: significant reduction in left anterior temporal CA dimensions (evidenced by red arrows), with subtle right deviation of midline structures and less thickness of left HS (evidenced by white arrows).
 | | | | Discussion | Most AC are usually asymptomatic, discovered as an incidental finding in neuroimaging studies, although rarely symptomatic cases are described, usually after minor traumatic brain injury.1,7 Our patient had a large AC that became symptomatic after a minor head injury that probably led to AC rupture with subsequent SH formation. SH causes an elevation in the intracranial pressure, which may lead to the appearance of symptoms such as headache, nausea, vomiting and rarely diplopia, secondary to VI cranial nerve palsy.2,7 Symptoms usually become severe for days or weeks after onset, but they eventually resolve.2,7 Physical findings are usually limited to papilledema, which was absent in our patient. Furthermore, history of minor trauma without loss of consciousness, verified in this clinical case, is described as a relatively common finding in the literature.1,7
The treatment approach of an AC with SH remains controversial and neurosurgical treatment was traditionally recommended, but newer reports have been questioning this strategy.1,7,8 There is no Class I evidence regarding the role and type of surgery for the treatment of these lesions.1 Conservative management has been proposed for patients who do not demonstrate signs of increased intracranial pressure or focal neurological signs, because of the surgery’s morbidity.1,7,8
Some authors suggest that AC should be treated if there is evidence of local mass effect on neuroimaging.7 However this can be potentially problematic in the context of SH, since any moderately sized SH and even many of the asymptomatic AC can produce the appearance of local mass effect on adjacent tissues.7
Recent articles have been highlighting the natural course of cyst-associated SH, even when symptomatic, that is usually benign and symptom resolution can be expected in most cases. Therefore, symptomatic SH is not considered an absolute indication for surgical treatment anymore and expectant management can result in good outcomes in many cases, even in the presence of intracranial hypertension symptoms.1,5,7,8
We must, therefore, weigh the risks and benefits of conservative versus surgical treatment in symptomatic patients on an empirical individual patient basis.1,5,7 There are still other important variables to consider in this equation: AC location, impact on CSF flow dynamics, symptomatic progression, risk of disfigurement due to bone remodeling (for large cysts), as well as presence of focal neurological deficits or focal seizures.5,8
Finally, this clinical case corroborates the most recent evidence, by illustrating the success of the conservative approach.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Jafrani R, Raskin JS, Kaufman A, Lam S. Intracranial arachnoid cysts: Pediatric neurosurgery update. Surg Neurol Int. 2019;10:15 [CrossRef] [PubMed] [PMC free article]
- Mazurkiewicz-Bełdzińska M, Dilling-Ostrowska E. Presentation of intracranial arachnoid cysts in children: correlation between localization and clinical symptoms. Med Sci Monit 2002; 8: CR462-465.
- Karnazes AC, Kei J, Le MV. Image Diagnosis: Arachnoid Cyst. Perm J. 2015; 19:e110-e111 [CrossRef] [PubMed] [PMC free article]
- Ben Dahman A, David P, Massager N, Leistedt S, Loas G. A marsupialized retrovermian arachnoid cyst and psychotic symptoms. J Surg Case Rep. 2017;2017:rjx162 [CrossRef] [PubMed] [PMC free article]
- Gosalakkal JA. Intracranial arachnoid cysts in children: a review of pathogenesis, clinical features, and management. Pediatr Neurol. 2002;26:93-98
- Guerrero-Fdez J, Sánchez AC, Bonis AB, et al. Manual de Diagnostico y Terapeutica en Pediatria 6ª ed, 2018 "Libro Verde. Hospital infantil La Paz"
- Maher CO, Garton HJ, Al-Holou WN, Trobe JD, Muraszko KM, Jackson EM. Management of subdural hygromas associated with arachnoid cysts. J Neurosurg Pediatr. 2013;12:434-443 [CrossRef] [PubMed]
- Filho SC, Marques JA, Albuquerque LA, et al. Cisto aracnóide intracraniano. Arq Bras Neurocir 2007; 26: 164-172. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2021.6
|
|