Torticollis
Ashok Johari
Consulting Pediatric Orthopedic, Bombay Hospital, B.J.Wadia Children's Hospital, Children's Orthopedic Centre, Mumbai, India.
First Created: 02/28/2001
Show details
Introduction
Torticollis is a rotational deformity of the neck, which may be seen at birth or may develop later.
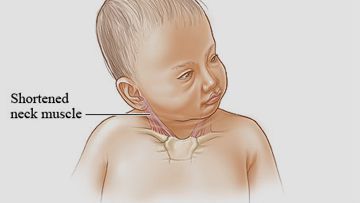
Congenital Torticollis
It results from fibromatosis of the sternomastoid and is seen up to 2 weeks after birth. The swelling is usually located near the clavicular attachment of the sternomastoid and at times, it involves the whole muscle. The usual course is one of spontaneous regression over a period of 1 year. Therefore treatment in infancy is purely conservative. Parents should be instructed to stretch the sternomastoid by manipulation, positioning in sleep, and play therapy. They should approach the baby and place toys on the side, which has a rotational limitation (the same side as the contracted sternomastoid) so that the baby is forced to turn its head thereby actively stretching the contracture. Any permanent torticollis becomes worse during growth and results in a deformity resistant to correction due to adaptive soft tissue and bony changes. The head inclines towards the affected side and face to the opposite side. The patient develops facial asymmetry, changes in the front-occipital diameter, and elevation of the ipsilateral shoulder. CDH or acetabular dysplasia is an association in up to 20% and careful screening for these is mandatory.
Non - operative treatment after one year is rarely successful. Operative treatment involves the release of tight soft tissues (the sternomastoid) followed by a period of casting and bracing to maintain the correction. Best results are obtained with the early operation - usually around one year of age. Regardless of the type of treatment - established facial asymmetry and limitation of motion greater than 300 at the start of treatment usually preclude a good result.
Acquired Torticollis
It is multifactorial. In children between 6 and 12 years of age, upper respiratory tract infection is a common cause. Patients develop a spontaneous atlantoaxial subluxation barely noticeable on radiographs. Treatment is by continuous cervical traction followed by collar wear till muscle spasm resolves. Tuberculosis of the atlantoaxial region with the subluxation is frequently seen in a pediatric orthopedic setting. Other causes include trauma with resultant subluxation or dislocation or a fracture-dislocation of the cervical spine, paralysis (post-polio), ocular disturbances, and rarely spasmodic torticollis.
1. Armstrong D, Pickrell K, Fettr B, Pitts W. Torticollis : an analysis of 271 cases. Plat Reconstr surg 1965, 35: 14.
2. Canale ST, Griffin DW, Hubbard CN. Congenital muscular torticollis : a long term follow up. J Bone Joint Surg 1982, 64-A.
3. Conventry MB, Harris L. Congenital muscular torticollis in infancy : some observations regarding treatment. J Bone Joint surg 1959, 41-A:815.
4. Hummer CD Jr, MacEwen GD. The coexistence of torticollis and congenital dysplasia of the hip. J Bone Joint surg 1972, 54-A: 1255.
5. Ling CM, The influence of age on the results of open sternomastoid to tomy in muscular torticollis. Clin Orthop 1976, 116: 142.
 Ashok Johari
Torticollis
https://www.pediatriconcall.com/show_article/default.aspx?main_cat=pediatric-orthopedics&sub_cat=torticollis&url=torticollis-introduction
2001-02-28
2001-02-28
Ashok Johari
Torticollis
https://www.pediatriconcall.com/show_article/default.aspx?main_cat=pediatric-orthopedics&sub_cat=torticollis&url=torticollis-introduction
2001-02-28
2001-02-28
×
Contributor Information and Disclosures
Ashok Johari
Consulting Pediatric Orthopedic, Bombay Hospital, B.J.Wadia Children's Hospital, Children's Orthopedic Centre, Mumbai, India.
First Created: 02/28/2001
×
References
1. Armstrong D, Pickrell K, Fettr B, Pitts W. Torticollis : an analysis of 271 cases. Plat Reconstr surg 1965, 35: 14.
2. Canale ST, Griffin DW, Hubbard CN. Congenital muscular torticollis : a long term follow up. J Bone Joint Surg 1982, 64-A.
3. Conventry MB, Harris L. Congenital muscular torticollis in infancy : some observations regarding treatment. J Bone Joint surg 1959, 41-A:815.
4. Hummer CD Jr, MacEwen GD. The coexistence of torticollis and congenital dysplasia of the hip. J Bone Joint surg 1972, 54-A: 1255.
5. Ling CM, The influence of age on the results of open sternomastoid to tomy in muscular torticollis. Clin Orthop 1976, 116: 142.