Irene Lieu1, Soyi Sarkar2, Kei U. Wong1.
1Rutgers New Jersey Medical School, Newark, NJ, USA,
2Georgetown Med-Star Hospital, Washington DC, USA.
ADDRESS FOR CORRESPONDENCE
Kei U. Wong, Rutgers New Jersey Medical School, Newark, NJ, USA.
Email: kei.wong@rutgers.edu | | Abstract | Background: Firearm injuries are the leading cause of death among children in the United States. Pediatric emergency departments (PEDs) offer an opportunity for injury prevention, though firearm safety interventions are not routinely implemented.
Objective: To evaluate the feasibility and impact of a PED-based firearm safety intervention using video education, gun lock distribution, and caregiver surveys.
Methods: We conducted an IRB-approved pilot study in a community PED in Newark, New Jersey (June 2025–February 2026). English-speaking caregivers of pediatric patients were recruited as a convenience sample. Participants viewed a 5-minute firearm safety video, were offered a gun lock, and completed a pre-survey assessing knowledge, beliefs, and behaviors. A follow-up survey was conducted at 6 months. Quantitative data were analyzed descriptively; qualitative responses were categorized into themes.
Results: Of 27 consented participants, 25 completed the pre-survey and 6 completed follow-up. Caregivers reported strong support for safe storage practices and clinician-led counseling, and most found the intervention acceptable and educational. At follow-up, 4 of 6 respondents reported increased inquiry about firearm storage in homes their children visit. Qualitative responses suggested increased awareness and behavior change.
Conclusion: A brief PED-based firearm safety intervention is feasible and well accepted, with preliminary evidence of improved caregiver awareness and behaviors. | | | | Keywords | Firearm safety, Harm Reduction, Gun trigger locks, Pediatric Emergency Department, Injury Prevention.
Abbreviations: Pediatric Emergency Department (PED). | | | | Introduction | Firearms injuries are the leading cause of death among children and adolescents in the United States, with most fatal incidents involving younger children occurring at home. Rates of unintentional firearm-related suicides and injuries continue to rise, disproportionately affecting Black children, males, and adolescents.1 Healthcare providers play a critical role in promoting child safety; each encounter with pediatric patients and their families, including visits to the pediatric emergency department (PED), represents a meaningful opportunity to discuss firearm safe storage.
Prior research demonstrates video-based education effectively influences health behaviors, including firearm safety practices in pediatric settings.2 Guided by this evidence, we implemented a firearm safe storage educational intervention in the PED to aid families in adopting safer home practices.
Supported by an internal institutional pilot grant, this study aims to assess the impact of a pilot harm-reduction educational intervention consisting of: 1) firearm safety video, 2) distribution of gun locks, and 3) pre-survey and post-survey assessing parents’ and guardians’ knowledge, beliefs, and practices related to firearm safety within a community PED. | | | | Methods & Materials | Study design and setting: We conducted this IRB-approved pilot study in the PED at University Hospital (Newark, New Jersey) from June 2025 to February 2026 to evaluate the impact of our firearm safety educational intervention.
Recruitment and participants: Families were recruited as a convenience sample during times when trained research staff were present in the PED. Eligible participants were parents/guardians (≥18 years) accompanying children (<18 years) presenting to the PED for any chief complaint (i.e., not limited to firearm-related injury visits).
Inclusion criteria: (1) parent/guardian present with the pediatric patient, (2) English-speaking, and (3) able to provide informed consent.
Exclusion criteria: Families were not approached when urgent clinical care or workflow constraints precluded safe/feasible consent and participation (e.g., active resuscitation or immediate procedures). Non–English-speaking caregivers were excluded because study materials were only available in English during this pilot.
Intervention Workflow: After informed consent, participants 1) viewed a 5-minute firearm safe-storage video created by Be SMART (Be Smart for Kids)3; 2) were offered a firearm safety device (gun trigger lock) during the PED visit; and 3) completed a survey assessment of caregiver knowledge, beliefs, and reported practices.
Survey Instrument: Participants completed an anonymous electronic survey assessing demographics, baseline beliefs and attitudes regarding firearm injury prevention, household firearm access/ownership, caregiver-reported practices, including frequency of asking about firearms in homes their children visit, and perceived knowledge gain/acceptability of the video and the gun lock. The survey instrument was developed by the study team based on clinical experience and review of relevant literature and was not derived from a previously validated instrument.
Follow-up: Approximately 6 months after the initial PED visit, participants with valid phone numbers were contacted for a follow-up survey using parallel items to assess disclosed practices and perceptions over time. Participants were contacted 1-5 times over 1 month, depending on whether they answered, requested a callback, or did not answer. Follow-up respondents were asked whether they were the same caregiver who completed the initial survey.
Analysis: The primary outcome was caregiver-reported firearm safety knowledge and behaviors. General qualitative themes were identified from free responses, and quantitative data were analyzed using descriptive statistics, including proportions and 95% confidence intervals (CIs). | | | | Results | A total of 27 patient families presented to PED consented and met inclusion criteria; 25 completed the pre-surveys and accepted the gun lock and were included in the analysis (25/27 = 92.6%).
At 6 months follow-up, 24 of the 25 initial participants were contacted, and the 1 remaining participant had not left a phone number. Of these, 6 completed the post-survey. Five phone numbers were no longer in service, and 13 participants either declined participation or did not answer.
Among the pre-survey cohort, pediatric patients ranged in age from 3 months to 17 years (mean age: 8.3 years); 62.5% were male, and 37.5% were female. Caregivers’ ages ranged from 24 to 61 years (mean 37 years), and 66% of caregivers were female. In the post-survey cohort, pediatric ages ranged from 6 months to 13 years (mean age: 5 years and 7 months); all children were male. Caregivers' ages ranged from 27 to 45 (mean 36 years), and 66% were female. All caregivers who completed the post-survey reported that they had also personally completed the pre-survey.
Most pre-survey caregivers endorsed the importance of gun safety devices, supported clinician-led firearm safety discussions, favored stricter firearm laws and background checks, and reported the video improved their knowledge. Specifically, 84% agreed/strongly agreed that gun owners should use firearm locking devices; 72% agreed/strongly agreed that healthcare providers should discuss firearm safety during medical encounters including ED visits; 68% agreed/strongly agreed that stricter gun laws decrease gun-related violence; 84% agreed/strongly agreed that background checks should be stricter; and 68% agreed/strongly agreed that the Be SMART video improved their learning/knowledge (Table 1). Opinions regarding the right to carry firearms remained mixed across survey responses (Figure 1).
Table 1. Percentage of Pre-survey and Post-survey Families in Support of Fire Safety Initiatives.
| Statement |
% Pre-survey agreed/strongly agreed |
% Post-survey agreed/strongly agreed |
| There should be stricter laws for background checks on guns/firearms |
84% (95% CI: 0.65 - 0.94) |
100% (95% CI: 0.61 - 1.00) |
| The video improved my learning about gun/firearm violence and injury prevention |
68% (95% CI: 0.48 - 0.83) |
83% (95% CI: 0.44 - 0.97) |
| Stricter gun laws will decrease gun-related violence and injuries |
68% (95% CI: 0.48 - 0.83) |
50% (95% CI: 0.19 - 0.81) |
| People should have the right to carry guns/firearms for protection |
36% (95% CI: 0.20 - 0.55) |
50% (95% CI: 0.19 - 0.81) |
| Healthcare providers should discuss gun/firearm safety during medical encounters including ED visits |
72% (95% CI: 0.52 - 0.86) |
83% (95% CI: 0.44 - 0.97) |
| Gun owners should all use gun/firearm locks devices (such as trigger locks or cables, gun lockboxes) |
84% (95% CI: 0.65 - 0.94) |
100% (95% CI: 0.61 - 1.00) |
Figure 1_Pre-survey to Post-survey Changes in Caregiver Inquiry regarding Firearms in Homes Children Visit.
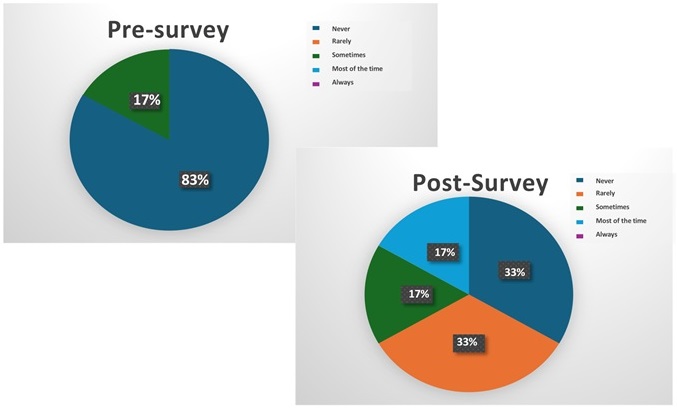
Pre-survey and post-survey changes in caregivers' reported frequency of inquiring about firearms in homes visited by their children, expressed as the percentage of respondents selecting each response category.
In the post-survey cohort, respondents reported continued endorsement of gun safety devices as helpful anticipatory guidance (Table 1). Although post-survey respondents reported not personally owning firearms, several described valuing having a gun lock for potential future firearm purchases or sharing with others in homes their children visit. One caregiver indicated they had recently received a permit to purchase a firearm and anticipated using the provided gun lock.
On follow-up, 4 of 6 caregivers reported asking about firearm storage in homes their children visit more often than they did before the PED visit (Figure 1). Qualitative responses suggested both the video and survey were educational, prompting reflection. The free-text responses were reviewed and grouped into recurring themes. One caregiver reported asking her child’s grandmother whether her firearm was secured and requested that the firearm safe not be opened with children present. | | | | Discussion | | Firearm sales and violence have surged markedly since 2020, accompanied by a substantial increase in pediatric firearm-related mortality. From 2019 to 2020 alone, firearm deaths among children increased by 30%.4 Black children and adolescents remain disproportionately affected, with mortality rates four times higher than those of their white counterparts.5 The continued post-pandemic escalation in firearm violence6, combined with the growing mental health burden and ease of access to firearms, is particularly concerning. | | | | Conclusion | | Pediatric emergency departments provide a valuable opportunity to promote firearm safety, especially in communities disproportionately affected by gun violence. Brief caregiver inquiry, educational videos, and gun lock distribution may improve safe storage. Pediatricians in all settings can advance firearm injury prevention as part of a broader public health initiative. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Naik Mathuria B, Cain CM, Alore EA, et al. Defining the full spectrum of pediatric firearm injury and death in the United States: It is even worse than we think. Ann Surg 2023;278:10-6. [CrossRef] [PubMed] [PMC free article]
- Silver AH, Azzarone G, Dodson N, et al. A randomized controlled trial for parents of hospitalized children: Keeping kids safe from guns. Hosp Pediatr 2021;11:691-702. [CrossRef] [PubMed]
- Be SMART Campaign. Be Smart for Kids. 2015. Available from: http://BeSmartForKids.org
- Centers for Disease Control and Prevention. CDC WONDER. 2021. Available from: https://wonder.cdc.gov/
- Martin R, Rajan S, Shareef F, et al. Racial disparities in child exposure to firearm violence before and during COVID-19. Am J Prev Med 2022;63:204-12. [CrossRef] [PubMed] [PMC free article]
- Mannix R, Lee LK, Fleegler EW. Coronavirus disease 2019 (COVID-19) and firearms in the United States: Will an epidemic of suicide follow? Ann Intern Med 2020;173:228-9. [CrossRef] [PubMed]
- Khubchandani J, Price JH. Public perspectives on firearm sales in the United States during the COVID-19 pandemic. J Am Coll Emerg Physicians Open 2021;2:e12293. [CrossRef] [PubMed] [PMC free article]
- Lee LK, Fleegler EW, Goyal MK, et al. Firearm-related injuries and deaths in children and youth: Injury prevention and harm reduction. Pediatrics 2022;150:e2022060070. [CrossRef] [PubMed]
- Donnelly MR, Grigorian A, Swentek L, et al. Firearm violence against children in the United States: Trends in the wake of the COVID-19 pandemic. J Trauma Acute Care Surg 2022;92:65-8. [CrossRef] [PubMed] [PMC free article]
- Campbell BT, Thaker S, Fallat ME, et al. A multicenter evaluation of a firearm safety intervention in the pediatric outpatient setting. J Pediatr Surg 2020;55:140-5. [CrossRef] [PubMed]
- Posner JC, Hawkins LA, Garcia-Espana F, et al. A randomized clinical trial of a home safety intervention based in an emergency department setting. Pediatrics 2004;113:1603-8. [CrossRef] [PubMed]
- Chaudhary S, Portugues A, Myers RK, et al. Paired video-based counseling and firearm safety device distribution in a pediatric emergency department. Acad Pediatr 2026;26:103168. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2027.57
|
| Cite this article as: | | Lieu I, Sarkar S, Wong K U. Promoting Gun Safety for Children and Families through the Pediatric Emergency Department. Pediatr Oncall J. 2026 Jun 29. doi: 10.7199/ped.oncall.2027.57 |
|