Shilpa Kalane1, N Kanade1, Usha Pratap2, Sanjay Gupte3.
1Division of Neonatology, Deenanath Mangeshkar Hospital and Deenanath Mangeshkar Hospital, Pune, Maharashtra, India,
2Pediatric Cardiology Division, Department of Pediatrics, Deenanath Mangeshkar Hospital, Pune, Maharashtra, India,
3Department of Obstetrics and Gynaecology, Deenanath Mangeshkar Hospital, Pune, Maharashtra, India.
ADDRESS FOR CORRESPONDENCE
Dr Shilpa Kalane, Division of Neonatology, 3rd floor, Superspeciality building, Department of Pediatrics, Deenanath Mangeshkar Hospital, Pune 04. Maharashtra, India.
Email: drshilpakalane@gmail.com | | Keywords | | atrial flutter, newborn, SVT | | | Atrial flutter (AFL) is an uncommon arrhythmia in newborns and infants. It is a form of supraventricular tachycardia (SVT) characterized by regular, rapid (atrial rates of 240 to 360 beats/min), “saw-toothed flutter waves,” often seen best in leads II, III, and aVF on the surface electrocardiograph (ECG). In neonates, 2:1 atrial conduction is common, resulting in a rate somewhat slower than typical paroxysmal SVT.
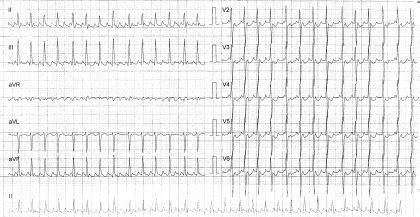
A male neonate, birth weight 3800 g, born at 36+4 weeks’ gestation by emergency caesarean section due to fetal tachycardia (heart rate 200 to 210 beats/min) was referred for further management. Antenatal history was not contributory. At birth, baby had tachycardia and inconsolable cry hence was referred. On admission, baby was euthermic, had heart rate >220 bpm, saturations in all 4 limbs were >95%, four limb blood pressure was normal and peripheral pulses were good. Blood sugar and ionic calcium level was normal. ECG showed SVT. Vagal maneuvers - ice pack application over eyeballs were performed. Baby received a dose of intravenous adenosine, resulting in a transient decrease in heart rate to 160 beats/min before increasing back to 200 to 210 beats/min. Repeat ECG showed atrial flutter (Figure 1). Cardioversion (0.5J/kg) was performed when hemodynamic instability developed. Rhythm normalized after successful cardioversion. Echocardiography and chest radiography were normal. Serum electrolytes and serum calcium and magnesium levels were normal. Baby was discharged on day 3. Presently baby is 6 months old and there is no recurrence.
Figure 1: ECG showing atrial flutter
The quoted incidence of SVT is estimated to be 1 in 100 for children of all ages and 1 in 200 to 250 for neonates. (1) Atrial tachycardia comprises 14% of SVT. (2) Atrial tachycardia includes atrial flutter (AF) and atrial ectopic tachycardia (AET). AF is an uncommon arrhythmia in newborns and infants. It is generally self-limited in infants who do not have heart disease. The low incidence of AF in this age group makes it difficult to study, and previous reports vary as to the most efficacious therapy and expected prognosis. (3,4) Arrhythmias in neonate can present with fetal tachycardia, non-immune hydrops or heart failure. In present case baby had fetal tachycardia and inconsolable cry. AF is a re-entrant tachycardia contained within the atrium. It may be difficult to differentiate the P waves; adenosine can be diagnostic if it unmasks the large, regular saw-tooth P waves. In present case adenosine unmasked AF. Congenital heart disease is reported in about 6.5% to 37% of neonates who have SVT. (1) In present case no cause was found. Baby responded to direct cardioversion. Literature mentions direct current cardioversion appears to be most effective at establishing sinus rhythm. (5) Atrial flutter in the absence of other arrhythmias has a low risk of recurrence. Once in sinus rhythm, infants with AF have an excellent prognosis and may not require chronic antiarrhythmic therapy. (5) This baby did not have underlying congenital heart disease, electrolyte imbalance or any other associated arrhythmia hence was not given any anti-arrhythmic agent.
Thus, we conclude that isolated AF in a newborn does not suggest an underlying structural heart defect. Infants with AF respond well to cardioversion. | | | | Acknowledgement | | Dr Sheela Patil (Respiratory therapist) for her guidance, Dr Arati Rajhans and Dr Rajan Joshi (HOD Pediatrics) for his guidance. | | | | Contributor Statement | | KS: search of the literature, partial English editing, and correction, KN: Final editing and correction, UP and GS: editing | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Garson A, Gillette P, McNamara D. Supraventricular tachycardia in children: clinical features, response to treatment, and long-term follow-up in 217 patients. J Pediatr. 1981;98:875–882. [CrossRef]
- Ko J, Deal B, Strasburger J, Benson D. Supraventricular tachycardia mechanisms and their age distribution in pediatric patients. Am J Cardiol. 1992;69:1028–1032. [CrossRef]
- Peng C, Chen M, Hou C, Hung H, Kao H, Hsu C, et al. Atrial flutter in the neonate and early infancy. Jpn Heart J 1998;39:287–95. [CrossRef] [PubMed]
- Mendelsohn A, Dick M, Serwer G. Natural history of isolated atrial flutter in infancy. J Pediatr 1991;119:386 –91. [CrossRef]
- Texter K, M, Kertesz N, Friedman R, Fenrich A. Atrial Flutter in Infants J Am Coll Cardiol. 2006 Sep 5;48(5):1040-6. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2016.14
|
| Cite this article as: | | Kalane S, Kanade N, Pratap U, Gupte S. Idiopathic Neonatal Atrial Flutter. Pediatr Oncall J. 2016;13: 23-24. doi: 10.7199/ped.oncall.2016.14 |
|