|
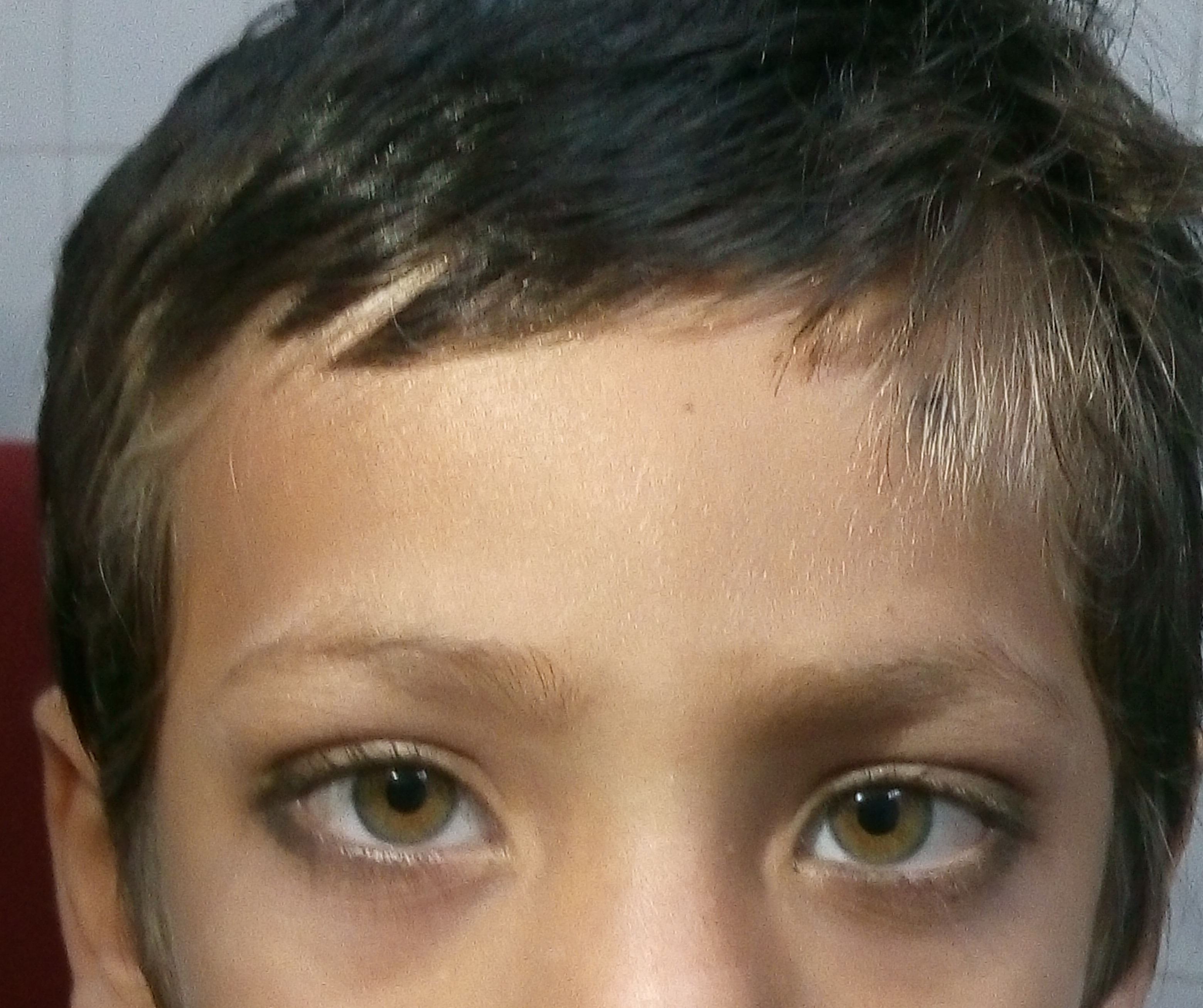
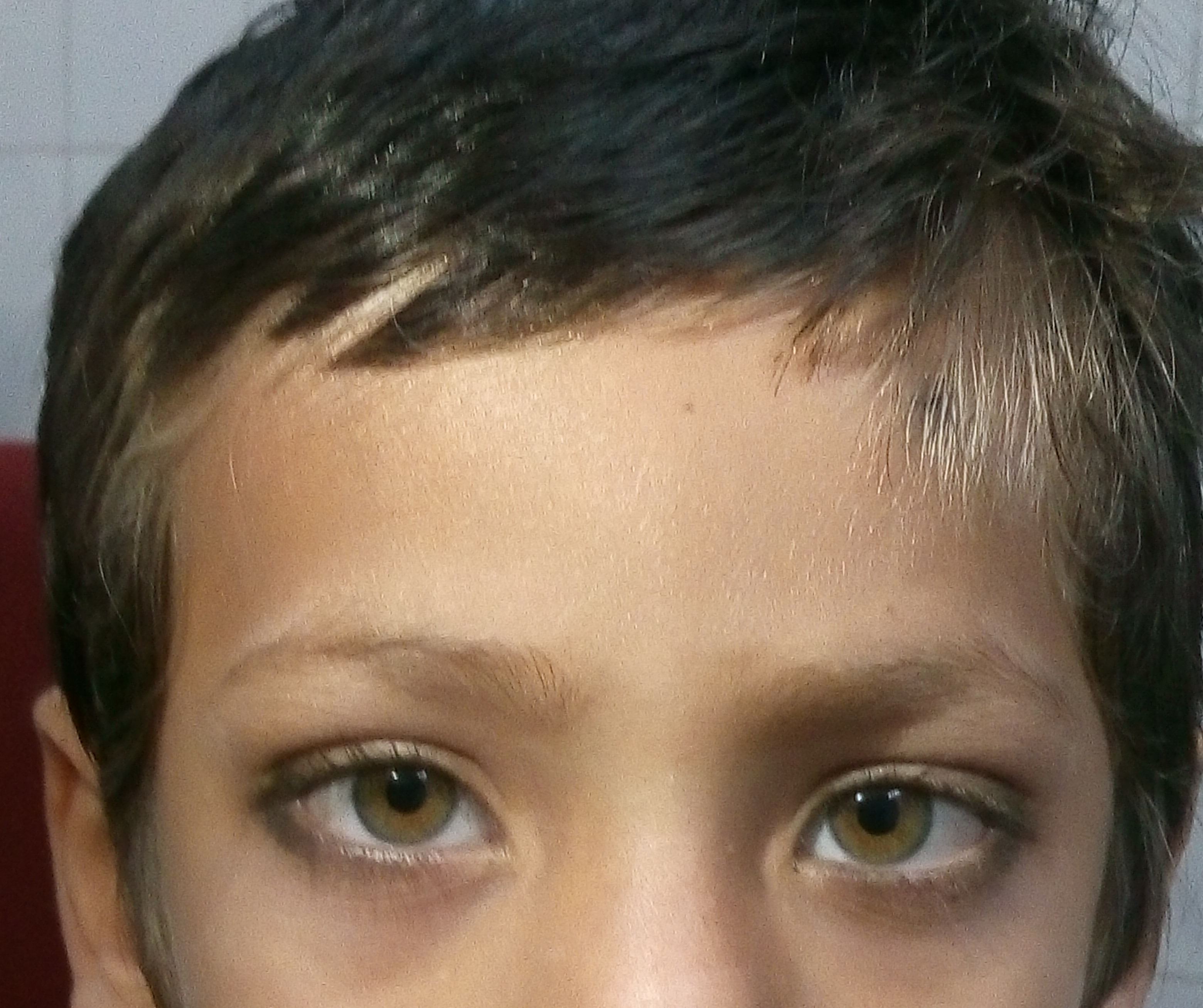
White lock of hair with heterochromia
Sanghamitra Ray, Prakash Chand Jain.
Department of Pediatrics, Cantonment General Hospital, Delhi Cantt, New Delhi.
ADDRESS FOR CORRESPONDENCE
Dr Sanghamitra Ray, Flat no- 176, DDA SFS flats, Pocket- 1, Sector-1, Dwarka. 1100075.
Email: dr.sanghamitra.ray@gmail.com
|
|
What is the diagnosis?
Clinically he was diagnosed as a case of Waardenburg Syndrome {WS} - a rare hereditary disorder with prevalence of 1 in 270,000 births that is characterized by the clinical manifestations of oculocutaneous anomalies of pigmentation, congenital deafness, dystopia canthorum, and broad nasal root. It can manifest with clinically heterogenous characteristics. There are at least four types of WS. Type I- persons usually have wide space between inner canthus. Hearing impairment occurs in 20 percent of cases. Type II- persons who do not have a wide space between inner canthus of their eye but have many other characteristics of WS are described in type I. However, 50 percent have hearing impairment or are totally deaf. WS type III is also known as Klein–WS. These patients have bony abnormalities including syndactyly, hypoplasia of the musculoskeletal system, flexion contractures, fusion of the carpal bones, winged scapulae. WS type IV is known as Shah–WS a rare combination of pigmentary abnormalities, hearing loss, and Hirschsprung disease. Most common are type I and II. It was first described by the Dutch ophthalmologist Petrus Johannes Waardenburg in 1951. As per the diagnostic criteria proposed by the Waardenburg consortium, a patient must have two major or one major plus two minor criteria to be diagnosed as WS type 1. {1} Major criteria include: Congenital sensorineural hearing loss, white forelock, hair hypopigmentation, pigmentation abnormality of the iris: complete heterochromia iridum {irides of different color} or partial, segmental heterochromia {two different colors in same iris, typically brown and blue}, hypoplastic blue irides or brilliant blue irides, dystopia canthorum, W index More than 1.95 and affected first-degree relative. Minor criteria include: skin hypopigmentation {congenital leukoderma}, synophrys, medial eyebrow flare, broad, high nasal root, prominent columella, hypoplastic alae nasi, premature gray hair {age Less than 30 years}. Our index case had three of the major criteria - white lock of hair, segmental heterochromia of iris and affected first degree relative {the elder female sibling}. Based on the above mentioned features, he was diagnosed as a case of Waardenburg syndrome type 1 {WS 1}. WS 1 is caused by loss of function mutation of PAX3 gene. {2} There is currently no cure for the syndrome. Being an autosomal dominant disease, WS-1 can recur in families and can have severe hearing impairment which is the most dreaded complication. So early diagnosis in the index case can help to detect all the affected family members and can even be offered genetic counselling and screening of the newborn babies for hearing impairment and offering them social and vocational training and rehabilitation if needed at the earliest. |
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
|
- Farrer LA, Grundfast KM, Amos J, Arnos KS, Asher JH Jr, Beighton P, et al. Waardenburg syndrome (WS) type I is caused by defects at multiple loci, one of which is near ALPP on chromosome 2: First report of the WS consortium. Am J Hum Genet 1992;50:902-13. [PubMed] [PMC free article]
- Wollnik B1, Tukel T, Uyguner O, Ghanbari A, Kayserili H, Emiroglu M, Yuksel-Apak M. Homozygous and heterozygous inheritance of PAX3 mutations causes different types of Waardenburg syndrome. Am J Med Genet A. 2003 Sep 15;122A(1):42-5. [CrossRef] [PubMed]
|
|
DOI: https://doi.org/10.7199/ped.oncall.2016.26 |
| |
Cite this article as:
Ray S, Jain P C. White lock of hair with heterochromia (Waardenburg syndrome). Pediatr Oncall J. 2016;13: 55. doi: 10.7199/ped.oncall.2016.26
|