KS Kumaravel, B Rameshbabu, KV Pugalendhiraja, NR Karthick, S. Santhoshkumar.
Government Dharmapuri Medical College, Dharmapuri, Tamilnadu, India.
ADDRESS FOR CORRESPONDENCE
Dr Kumaravel KS, Government Dharmapuri Medical College, Dharmapuri, Tamilnadu, India.
Email: kumaravelks@rediffmail.com | | Abstract | Introduction: The spectrum of gender discrimination against female children in health care ranges from nutritional denial to cruel forms like female infanticide. The practice of female infanticide was seen particularly in South Asian countries. In the late 1980s, it reached dangerous levels in certain districts of Tamilnadu with a falling child sex ratio. To check the practice of female infanticide, the government of Tamilnadu launched Cradle Baby Scheme in the state. This study analyses the clinico-social profile of babies saved under the scheme and reviewed the current status of child sex ratio in Dharmapuri and the interventions done by the state government against female infanticide.
Methodology: This is a retrospective descriptive study done at Cradle Baby Reception Centre of Government Dharmapuri Medical College Hospital, Dharmapuri from the year Jan 2002 to Mar 2016.
Results: Out of the 1363 babies rescued, 192 (14.1%) were preterm, 1125 (88%) were of birth order of 3 and above and in 1226 (90%) of cases the girl baby was given to the scheme by the parents. Poverty and female sex of the baby were cited as the most common cause of abandoning. Thirty-four (2.5%) babies had congenital anomalies and sepsis and prematurity were the common morbidities seen. Seventy-two (5.2%) girls were taken back by the parents and 1286 (94.4%) girls were handed over to social welfare department from where they were given for adoption.
Conclusion: The Cradle baby Scheme of Government of Tamilnadu has saved 1363 girl babies in this centre. Similar interventional strategies should be planned across the country in areas with low Child Sex Ratio. | | | | Keywords | | Cradle Baby Scheme, Child Sex Ratio, Female Infanticide, Dharmapuri | | | | Introduction | The spectrum of gender discrimination against girl children in health care ranges from nutritional denial, delayed medical care and emotional deprivation to more cruel forms like female infanticide and feticide. All of these were documented as causes leading to increased mortality in female children. Excess female child mortality has been reported mainly from South Asian countries. (1) The practice of female infanticide was common in China in the past and it was thought to be eradicated after the communist revolution. But in the recent years there are again reports of female infanticide in China, following the adoption of the 'One-Child' policy. (2) In addition, the female infanticide was also prevalent in Indian Diasporas settled elsewhere like in Canada. (3)
During the late 1970s, cases of female feticide were reported from many cities of India. (4) The gender discrimination and female infanticide in Tamilnadu were less reported and there are very little data till 1980s. During the 19th century the British reported the presence of female infanticide in Tamil Nadu among certain communities, which provides evidence of its existence as early as 19th century in Tamilnadu. (5) During late 1980s researchers reported a large quantum of missing girl children during their nutritional survey in northern Tamilnadu. (6) A 1995 study of 1320 newly delivered women in northern districts of Tamilnadu found that the number of girls who died in the neonatal period was three times that of boys - a statistically significant difference. The risk was even more increased among female children born to multiparous women without male children. (7) The risk of neglect is also high among girls of high birth order, according to studies in North India, Pakistan and Bangladesh. (8)
In the early 90’s, Salem and Dharmapuri districts of Tamilnadu were in the global news as the female infanticide came to public attention as the Child Sex Ratio (the number of girls per 1000 boys under the age of 5 years) reached alarmingly low levels in these districts. At that time the state government initiated many measures to check this practice. Amongst the various schemes introduced for the welfare of female children, the “Cradle Baby Scheme” which was introduced in Salem during 1992 was the most important one. (9) This scheme was aimed at eradicating the practice of female infanticide. Under this scheme, cradles were placed in important places such as hospitals, primary health centres and child care homes where the parents can leave their unwanted female children. Female children found abandoned at public places were also rescued.
The government of Tamilnadu concurrently launched many interventions to reduce female infanticide. The Chief Minister’s Girl Child Protection Scheme was launched in 1992 and the goal of the scheme was elimination of female infanticide by the year 2000. (9) Under the scheme, a poor family with one or two girls and no sons would be eligible for monetary incentives. Money given in the name of the infant girl would be held in a fixed deposit account until she reached 21 years of age. Further, when the girl went to school, the family would periodically receive grants for educational expenses. The Pre Natal Diagnostic Technique Act introduced in 1994 and was later amended in 2003 as Pre Conceptional & Pre Natal Diagnostics Techniques Act 2003 and more powers were delegated to punish the perpetrators of female feticide. (9)
The Cradle Baby Scheme was revitalized in 2001, by setting up full-fledged reception centres at 4 other places of Madurai, Theni, Dindigul and Dharmapuri. In the reception centres adequate staff, equipment like warmers, incubators, lifesaving drugs, refrigerators and facilities like gas stove connection, essential vessels and telephone connection were provided. Children rescued under the Cradle Baby Scheme were rehabilitated with an alternate family under adoption programs. The differently abled children were sent to Special Homes run by Non-Governmental Organizations for rehabilitation.
Though many social and political studies about the female infanticide are available, there is not even a single study available describing the social and clinical profile of the children who survived the infanticidal practice. This study is aimed at providing clinical and social profile of the children admitted under Cradle Baby Scheme. | | | | Methods & Materials | Objectives:
1. To study the clinical and social profile of the babies admitted in the cradle baby reception centre of Government Dharmapuri Medical College Hospital, Dharmapuri.
2. To review the current status of Child Sex Ratio in Dharmapuri district
| | | | Methodology | | This is a retrospective descriptive study done at Cradle Baby Reception Centre of Government Dharmapuri Medical College Hospital, Dharmapuri from the year Jan 2002 to Mar 2016. The universal sampling method was employed. Clinical and social data like age of the baby, birth order, gestational age, reason for abandoning, abandoner, morbidity pattern and the outcome were recorded from the case records and were tabulated. Standard case definitions were used for gestational age assessment and neonatal morbidities. Descriptive analysis was done using Microsoft excel. Since few of these children were abandoned in public places, data regarding their birth order, reason for abandonment and abandoner could not be obtained. So their demographic and social aspects could not be studied. For the purpose of review of current status of Child Sex Ratio and the state government interventions against female infanticide, the policy document of Social Welfare Department of Government of Tamilnadu was considered. (9) | | | | Results | There were totally 1363 girl babies rescued and admitted in the scheme since its inception in the hospital. In the initial few years there were more than 100 babies rescued every year. In the recent years, number of abandoned cradle babies is showing a declining trend (Fig 1). Clinico-social profile of these babies is depicted in Table 1. The oldest baby received was aged 3½ years. In our study, there were 63 first born babies who were abandoned. The reason for abandoning of the first born babies were illegitimacy in 27 girls, congenital anomaly in 22 girls and it was female sex of the baby being the sole reason in the rest. The congenital anomalies observed in the study include cleft palate/cleft lip in 9 (26%) babies, neural tube defects in 4 (11%) babies, ano-rectal malformations in 4 (11%) babies, and hydrocephalus in 1 (3%) baby and other anomalies in the rest. In the study group, 5 babies died of which sepsis was the cause in 2 babies, congenital anomaly in 1 baby and prematurity in 2 babies.
Figure 1: ANNUAL ADMISSIONS
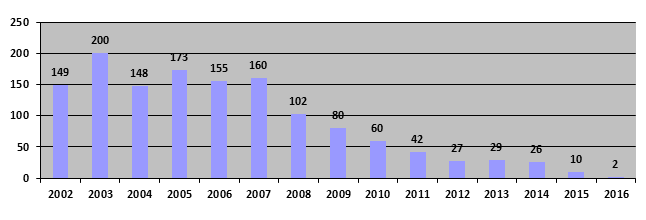
Table 1: Clinico-social Profile of the Babies
| Gestational age of the babies (n=1363) |
Term: 1171 (85.9%)
Preterm: 192 (14.1%) |
| Age at the time of abandoning |
< 1 week: 984 (72.2%)
1-4 weeks: 308 (22.6%)
> 4 weeks: 71 (5.2%)
|
| Birth order of the babies |
1st born: 63 (5%)
2nd born: 84 (7%)
3rd born: 698 (55%)
4th and above: 427 (33%)
|
| Cause of abandoning |
Poverty: 421 (33%)
Illegitimacy: 27 (2%)
Female sex of the child 790 (62%)
Congenital anomalies 34 (3%)
|
| Abandoner |
Abandoned at public places: 137 (10.05%)
Parents: 1226 (89.95%)
|
| Morbidity Pattern |
Sepsis: 18 (20.5%)
Bronchopneumonia 34 (38.6%)
Malnutrition 4 (4.5%)
Morbidity due to congenital anomalies: 16 (18.2%)
Morbidity due to prematurity: 16 (18.2%)
|
| Outcome |
Handed over for adoption: 1286 (94.4%)
Taken back by parents: 72 (5.2%)
Died: 5 (0.4%) |
| | | | Discussion | In our study, we found that as the birth order increased, the abandoning of female infants also increased. Many other studies in South Asia and North India reported a similar trend in female infanticide. (8,10) Muhari et al reported that up to 80-90 percent of victims of female infanticide are girls of higher birth order (possibly greater than 2). (8) Apart from female infanticide, the risk of neglect of girls who survive is also high among girls of high birth order, according to studies in North India, Pakistan and Bangladesh. (10) In this study, poverty and female sex of the baby were the cited as the common reasons for abandoning female children. There are many studies available which reported the following factors as responsible for the increase in the incidence of female infanticide: the low status of females as against males, decreasing family size and consequent intensification of son preference and widespread practice of dowry across all the caste groups in India. (6-8) In our study we observed that 2.5% babies had congenital anomalies and congenital anomalies might be the main reason for abandoning these babies. None of the studies have reported congenital anomaly as a reason for infanticide.
We observed in our study, 72 parents reclaimed their babies after a change of mind. Hence the parents may be given a second chance for reclaiming their babies before finally giving them to adoption agencies. Further studies are needed to ascertain the mindset of the parents regarding this.
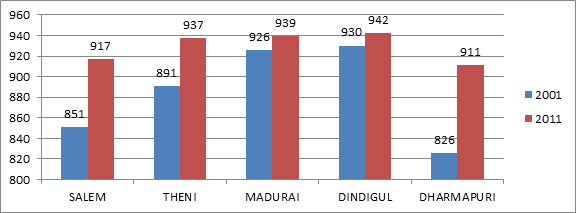
When the scheme was inaugurated in the year 1992, there were criticism saying that it would encourage the parents to abandon the female babies and would not be a substitute for tackling the crime of sex selection and female feticide. But the greatest proof for the impact of Cradle Baby Scheme on survival of female infants is evidenced by the improving CSR in the districts where it was operational. We noticed a decreasing trend in the number of abandoned cradle babies over a period of years in our study. This correlates with an improving CSR in the district – from 826 in 2001 to 911 in 2011. (9) It can be noted that in the five districts where the Cradle Baby Scheme has been in operation, the Child Sex Ratio has shown a positive trend as seen in Fig 2, whereas the overall Child Sex Ratio of Tamil Nadu state which was 942 per 1000 males during 2001, increased to 946 during 2011.(9)
Fig 2: Child Sex Ratio of Districts Where Cradle Baby Scheme was Operational (9)
 | | | | Conclusion | | The Cradle baby Scheme of Government of Tamilnadu has saved 1363 girl babies in this centre. Similar interventional strategies should be planned across the country in areas with low Child Sex Ratio. | | | | Acknowledgement | | We sincerely thank the Staff nurses, pediatricians, department of social welfare and Government of Tamilnadu who helped for this study. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Ravindran TKS. Health implications of gender discrimination in childhood: unraveling the complexities. World Health Organization, Geneva, 1997.
- Krist of ND. Peasants of China discover new ways to weed out girls. New York Times. 21st July 1993.
- Stephen JD. Sexing the fetus. Cases of female infanticide are sensationalised by the media in Canada. Lancet. 1991; 338:1336.
- Ramanamma A, Bambawale U. The mania for sons: an analysis of social values in South Asia. Soc Sci Med Med Anthropol. 1980;14(2):107-10. [CrossRef]
- George SM, Abel R, Miller BD. Female infanticide in South Indian villages. Economic and Political Weekly. 1992; 27:1153.
- George SM. Female Infanticide in Tamil Nadu, India : From Recognition Back to Denial? Reproductive Health Matters 1997;10:124-132. [CrossRef]
- Nielsen BB, Liljestrand J, Hedegaard M, Thilsted SH, Joseph A. Reproductive pattern, perinatal mortality, and sex preference in rural Tamil Nadu, South India: community-based, cross-sectional study. BMJ. 1997; 314: 1521-24 [CrossRef] [PubMed] [PMC free article]
- Muhuri PK, Preston SH. Effects of family composition on mortality differentials by sex among children in Matlab, Bangladesh. Population & Development Review. 1991; 17:415-34. [CrossRef]
- Social welfare and nutritional meal programme department policy note 2015-2016. Govt of Tamilnadu 2015. Available at URL: http://cms.tn.gov.in/sites/default/files/documents/swnmp_e_pn_2015_16.pdf. Accessed on 1st June 2016
- Kielmann AA, Taylor CE, DeSweemer C, Uberoi IS, Takulia HS, Masih N, et al. The Narangwal experiment on interactions of nutrition and infections : II. Morbidity and mortality effects. Indian J Med Res. 1978;68 Suppl:21-41. [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2016.29
|
| Cite this article as: | | Kumaravel K, Rameshbabu B, Pugalendhiraja K, Karthick N, Santhoshkumar S. Profile of Babies Admitted in Cradle Baby Scheme and Review of Female Infanticide in Dharmapuri. Pediatr Oncall J. 2016;13: 40-43. doi: 10.7199/ped.oncall.2016.29 |
|