Shashidhar A, Suman Rao PN, Joe Jose.
Department of Neonatology, St John’s Medical College, Bangalore, India.
ADDRESS FOR CORRESPONDENCE
Dr Shashidhar A, Department of Neonatology, St John’s Medical College, Bangalore, India.
Email: shashiishere@gmail.com | | Abstract | Background: Downes` Score (DS) and Silverman Anderson Score (SAS) are widely used for the categorization of respiratory distress in neonates. However there are no comparative studies between them.
Aim: This observational study in a tertiary care neonatal intensive care unit (NICU) was conducted to compare the DS and SAS in preterm neonates with respiratory distress as assessed by interns and nurses.
Methods: After initial training, the subjects were made to assess newborns with respiratory distress using both the scores sequentially under observation of an expert. The scores given were compared for accuracy and correlated using Spearman rho test.
Results: The inter rater reliability was higher in DS (alpha=0.69- acceptable) as compared to SAS (alpha=0.33- questionable). DS showed fair agreement (ICC-0.51) while that of SAS was poor. (ICC-0.19). Mean score for ease was 3 for DS compared to 5.5 in SAS.(p=0.011). Conclusion: DS was found to have better accuracy, reliability and easier to use by primary health personnel. | | | | Keywords | | respiratory distress syndrome, newborn | | | | Introduction | Respiratory distress occurs in about 7% of all newborns (1) and is one of the commonest causes of neonatal intensive care unit (NICU) admissions worldwide accounting for about 30-40% of all admissions. (2) It is associated with high morbidity and mortality if not addressed appropriately.
Downes` score (DS) (3) and Silverman Anderson score (SAS) (4) are commonly used for quick diagnosis of distress and assessment of its severity. This grading is crucial in decision making for further management which might include mechanical ventilation for severe distress. DS is used for assessment of both term and preterm newborns whereas SAS has been validated only in preterm babies. However, to the best of our knowledge there has been no head to head comparison between the two scores and they continue to be used interchangeably in preterm newborns. The primary objective of this study was to compare the DS & SAS in preterm neonates with respiratory distress as assessed by interns and nurses. We also determined the accuracy of their scoring and the ease and time taken for assessment | | | | Methodology | The comparative observational study was undertaken in a tertiary care newborn unit at St. John’s Medical College, Bangalore between December 2015 to February 2016. We included interns who had completed their compulsory 7-day rotation in the department of neonatology and staff nurses who were working in the unit as study subjects by purposive sampling after taking written informed consent. Downes` score is part of the routine training of nurses and interns. The subjects were called to the unit whenever there was a preterm newborn (born at a gestational age of <37 weeks) with respiratory distress due to any cause but not on invasive ventilation or having acute hemodynamic instability. The participants were trained using a mannequin and a video on how to use both the scores by the co-investigator. They were then asked to assess the preterm infant for respiratory distress using both the scores sequentially. For half the subjects it was DS first followed by SAS and vice versa to avoid bias. The time taken for these assessments were noted. The co-investigator stood by the same baby’s bedside and concurrently assessed the same scores in the same order along with the participant. The scores given for each parameter by the 2 observers and the total scores were recorded. A maximum of 2 subjects were allowed to assess a single baby. The participants were then asked to rate the 2 scores for the ease of assessment on a scale of 1 to 10 with 1 being extremely easy and 10 being extremely difficult.
Purposive sampling was followed and a formal calculation was not attempted.
Statistical analysis: The scores given were analyzed by Spearman rho correlation and single measures intra class correlation coefficient (ICC) for inter observer reliability. The accuracy was also assessed against the co-investigator in terms of percentages. The exact score being taken as accurate and scores given more or less than the co-investigator being labelled as overscoring and underscoring respectively. The time taken by the participant for each assessment was compared using paired t test. The subjective ease of scoring was analyzed by chi square test & a p value of <0.05 was considered statistically significant. Analysis was done using SPSS v.20. | | | | Results | There were a total of 40 participants (20 interns and 20 nurses) in the study providing us with 80 scores and 80 scores by the investigator. There was no correlation between DS and SAS for a given severity of distress (p=0.237, r=0.189). (Fig 1) DS by interns and by nurses also correlated well with the investigator (r =0.36-low positive, and r =0.71-high positive respectively), while SAS correlated well among only nurses (r =0.485-low positive) but not with the interns (r = -0.06 - negligible). (Table 1)
The inter rater reliability was higher in DS (α=0.69- acceptable) as compared to SAS (α=0.33- questionable). DS showed fair agreement (ICC-0.51) while that of SAS was poor. (ICC-0.19) All the participants took significantly lesser time in evaluating newborns using DS (155.9±43 sec) compared to SAS (212.6±63 sec) (p<0.001). (Figure 2) The subjective ease of assessment was better in DS with mean score of 3 compared to SAS with a mean score of 5.5 (p=0.011).
Fig.1: Scatter plot showing comparison of DS and SAS
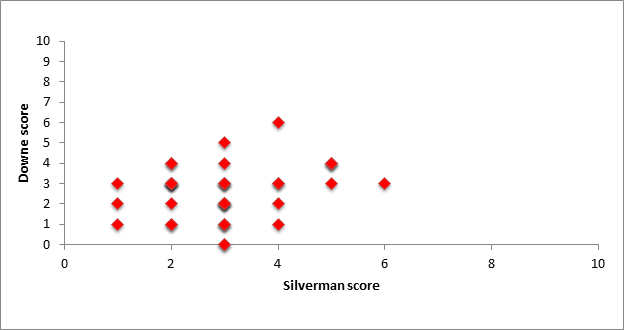
Fig 2: Chart showing mean time taken to score in seconds
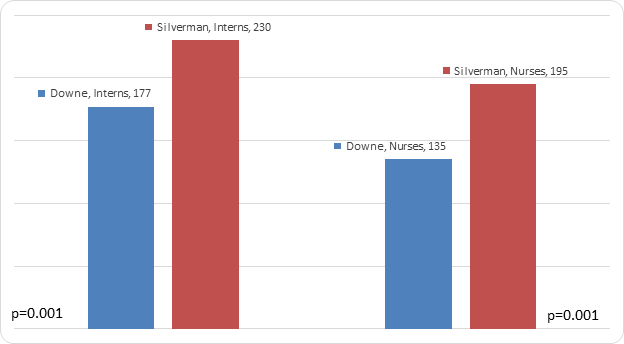
Table 1: Showing the accuracy of scores by subjects compared to investigator expressed as percentage
| Score |
|
Downes’ Score |
Silverman Anderson score |
| Interns |
Accurate |
33% |
10% |
| |
Over scored |
27% |
30% |
| |
Under scored |
40% |
60% |
| Nurses |
Accurate |
30% |
28% |
| |
Over scored |
25% |
19% |
| |
Under scored |
50% |
55% |
| | | | Discussion | The DS and SAS were devised for assessment of respiratory distress primarily in preterm babies with respiratory distress syndrome which has been extrapolated to other etiologies. (3,4) SAS, initially known as “retraction score” correlated well with mortality and DS with blood gas parameters with a sensitivity of 88% and a specificity of 81% in detecting hypoxemia. (5) The absolute values dictate the severity and need for ventilation (if either score is >6). Choice of the score in each NICU is usually based on personal preference and unit culture in the absence of evidence for superiority of either of the scores.
In this small study we attempted to compare the 2 scores as used by primary health care workers (interns & nurses) for accuracy, reliability and ease of use as these parameters have not been addressed previously in literature. Interns and nurses were chosen as they are likely to be the point of initial contact for sick newborns. These primary health care providers are also expected to make management decisions based on findings like respiratory distress including referral in various community health programs. Scoring of distress tries to add objectivity to a subjective assessment and increases standardization and improves documentation of progression of disease. However, for better retention and applicability the scoring has to be not only valid and reliable but also simple and easy to administer.
In our center, we have been using only DS for both term and preterm babies and found it to be simpler to train, better accepted and reproduced even in emergencies. In this study we have found that DS was not comparable to SAS when assessed by primary health care givers which may be due to the fact that SAS has many subjective elements like retractions and may require further intensive training for its accurate assessment. DS had lesser inter observer variability probably as the score is routinely used in the unit. It was easier to administer and needed lesser time of about a minute which maybe crucial for decision on referral for ventilation in community settings. SAS had significant underscoring (more than half the observations) as compared to DS which can adversely affect treatment decisions like babies being denied CPAP or ventilation even when deserved especially if facilities for pulse oximetry and blood gas analysis are unavailable.
The limitations in our study were the small sample size which may reduce the power of the study and not being able to assess babies with severe respiratory distress who would be invasively ventilated already. The presence of the co-investigator could have added to the pressure of the assessors but is likely to be equal during both the assessments. There could also be a selection bias as our unit has been using DS. | | | | Conclusion | | In our study, DS was found to be better than SAS for assessment of respiratory distress in preterm newborns and has better accuracy, reliability and easier to use by primary health personnel. This may be utilized in training programs for primary health care givers. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Kumar A, Bhat B V. Epidemiology of respiratory distress of newborns. Indian J Pediatr. 1996;63:93–98. [CrossRef] [PubMed]
- Guha D. NNF Recommended Basic Perinatal-Neonatal Nomenclature. In: Neonatology- Principles and Practice. 1998. p. 131–2.
- Downes JJ, Vidyasagar D, Boggs TR, Morrow GM. Respiratory distress syndrome of newborn infants. I. New clinical scoring system (RDS score) with acid--base and blood-gas correlations. Clin Pediatr. 1970; 9:325–331. [CrossRef] [PubMed]
- Silverman WA, Andersen DA. A controlled clinical trial of effects of water mist on obstructive respiratory signs, death rate and necropsy findings among premature infants. Pediatrics. 1956;17(1):1–10. [PubMed]
- Rusmawati.A, Haksari EL, Naning R. Downes score as a clinical assessment for hypoxemia in neonates with respiratory distress. Paediatr Indones. 2008;48:342-5. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2016.30
|
| Cite this article as: | | A S, PN S R, Jose J. Downes Score vs Silverman Anderson Score for Assessment of Respiratory Distress in Preterm Newborns. Pediatr Oncall J. 2016;13: 66-68. doi: 10.7199/ped.oncall.2016.30 |
|