Jamal Ahmed Omer.
Department of General Pediatric, King Fahad Medical City, Riyadh, Saudi Arabia.
ADDRESS FOR CORRESPONDENCE
Dr Jamal Omer, Department of General Pediatric, King Fahad Medical City, Riyadh, Saudi Arabia.
Email: dr.jamal.001@gmail.com | | Abstract | | Most patients with coarctation of the aorta present with hypertension and congestive cardiac failure. We report a five months old male infant who presented with breath holding spells (pallid) due to post-ductal coarctation of the aorta which was resolved after dilation. | | | | Keywords | | Coarctation of Aorta, Breath holding, infant, Child | | | | Introduction | | Coarctation of the aorta accounts for 4 to 6 percent of all congenital heart defects with reported prevalence of 4 per 10,000 live birth. (1) Most of the cases are sporadic. Patients often present with hypertension, a murmur and congestive heart failure. Diagnosis is made after hypertension is noted as an incidental finding during eval-uation of other problems. Occasionally child may experience pain or weakness in the legs. (2) We present an infant who presented with breath holding spells due to coarctation of the aorta. | | | | Case Report | A 5-month-old boy presented with shortness of breath for 15 days which was associated with perioral cyanosis and breath holding for seconds associated with pallor of the face. He was born late preterm by cesarean section and was in the neonatal intensive care unit (NICU) for 25 days due to patent ductus arteriosus (PDA), which closed without surgical intervention. For the current episode, he was hospitalized for seven days and treated as bronchiolitis. Five days after discharge, the mother noticed reoccurrence of the same episodes. On presenta-tion to us, general examination was normal. All pulses were felt and 4 limbs blood pressure was normal. On car-diovascular system examination, systolic murmur was present at the apex. Investigations in form of complete blood count, renal function tests and blood culture were normal. ESR was 94mm; at end of 1 hour, Respiratory viral panel initially was positive for rhinovirus, which became negative after 2 weeks. Chest X-ray revealed bilat-eral hyperinflation with normal heart. Echocardiography initially revealed small atrial septal defect (ASD) with possibility of coarctation of the aorta. CT of the great vessels showed mild post-ductal distal coarctation of the aorta. (Figure 1 and 2) Cardiac catheterization and balloon dilatation was done to dilate the stenotic part. After the cardiac catheterization, the patient was observed for 6 days and there were no documented breath holding spells.
Figure 1. 3D CT angiogram which demonstrates post-ductal coarctation of the aorta

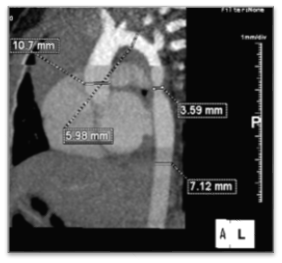
Figure 2. CT angiogram which revealed post-ductal coarctation of the aorta
| | | | Discussion | Breath holding spells are common events in infants and young children from six months to six years of age. (3) Most children (80 to 90 percent) with these spells have their first episode before 18 months of age. The two clinical types of breath-holding spells are cyanotic and pallid. Family members can demonstrate both types, but usually one predominates. (4) Pallid breath-holding spells result from exuberant vagally-mediated cardiac inhibition. (3) It is less common than cyanotic one. The child typically loses consciousness after a minor fall or blow to the head or upper body. (3) Often, this history is not volunteered by the patient or family. The child then stops breathing and becomes pale, diaphoretic, and limp. Other causes of syncope also should be consid-ered if the episodes are prolonged or frequent, precipitated by startle or other non-traumatic stimuli, or if a family history of syncope or sudden death exists, a more in-depth cardiac evaluation, is indicated.
In literature review such presentation of coarctation of the aorta were not found. There are some cases reported for coarctation of the aorta with unusual presentations. There was an infant with aortic coarctation who presented with a severe degree of myocardial dysfunction similar to “cardiomyopathy” and who was suc-cessfully treated by balloon angioplasty, with restoration of normal left ventricular size and function. (5) Stridor can be the sole presenting feature of the aortic coarctation resulting from enlargement of the innominate ar-tery, which severely compress the anterior tracheal wall. (6) Although coarctation may cause enlargement of systemic arteries (e.g. intercostal vessels causing rib notching), aneurysmal dilatation of the subclavian or innominate artery which resolved following resection of the juxtaductal aortic coarctation and aortopexy has been reported in a case report. (7) Abnormal aortic arch development and vascular compression of the trachea may also elicit turbulent airflow in the central airways and produce stridor, wheeze, ‘recurrent croup,’’ recur-rent pneumonia/bronchitis, and reflex apnea. (8,9) In our patient, we assume that the breath holding spells may have been secondary to pain. Since he had a mild coarctation, his blood pressure and pulses were normal.
In conclusion, coarctation of aorta in children could present with unusual symptoms and one should al-ways rule out coarctation of aorta in a child with breath holding spell. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol 2002; 39:1890. [CrossRef]
- Ing FF, Starc TJ, Griffiths SP, Gersony WM. Early diagnosis of coarctation of the aorta in children: a continu-ing dilemma. Pediatrics. Sep 1996;98(3 Pt 1):378-82. [PubMed]
- Breningstall GN. Breath-holding spells. Pediatr Neurol. 1996; 14:91. [CrossRef]
- DiMario FJ Jr. Prospective study of children with cyanotic and pallid breath-holding spells. Pediatrics 2001; 107:265. [CrossRef]
- Salahuddin N, Wilson AD, Rao PS. An unusual presentation of coarctation of the aorta in infancy: Role of balloon angioplasty in the critically ill infant. Am Heart J. 1991;122:1772–1775. [CrossRef]
- Park JG, Wylam M. Congenital Stridor: Unusual Manifestation of Coarctation of the Aorta. Pediatr Cardiol. 2006;27:137–139. [CrossRef]
- Schneeweiss A, Blieden LC, Shem-Tov A, et al. Coarctation of the aorta with congenital hemangioma of the face and neck and aneurysm of dilatation of a subclavian or innominate artery. Chest.1982; 82:186–187. [CrossRef]
- McLaughlin RBJ, Wetmore RF, Tavill MA, Gaynor JW, Spray TL. Vascular anomalies causing symptomatic tra-cheobronchial compression. Laryngoscope.1999; 109:312–319. [CrossRef]
- Moes CAF, Izukawa T, Trusler GA. Innominate artery compression of the trachea. Arch Otolaryngol.1975; 101:733–738. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2017.36
|
| Cite this article as: | | Omer J A. Unusual Presentation of Coarctation of the Aorta in a 5-month-old Infant. Pediatr Oncall J. 2017;14: 88-89. doi: 10.7199/ped.oncall.2017.36 |
|