Neha Agarwal, Sunil Taneja, Ayank Tandon.
Department of Pediatrics, GSVM Medical College, Kanpur, Uttar Pradesh, India.
ADDRESS FOR CORRESPONDENCE
Dr Sunil Taneja, 113/159 A Swaroop Nagar, Kanpur 208002, Uttar Pradesh, India.
Email: tanejasunil17@gmail.com | Achondroplasia is the most common skeletal dysplasia in children. Midface hypoplasia and skull base deformities predispose these children to sleep disordered breathing (1) and increase the risk of upper airway obstruction during sleep. (2,3)
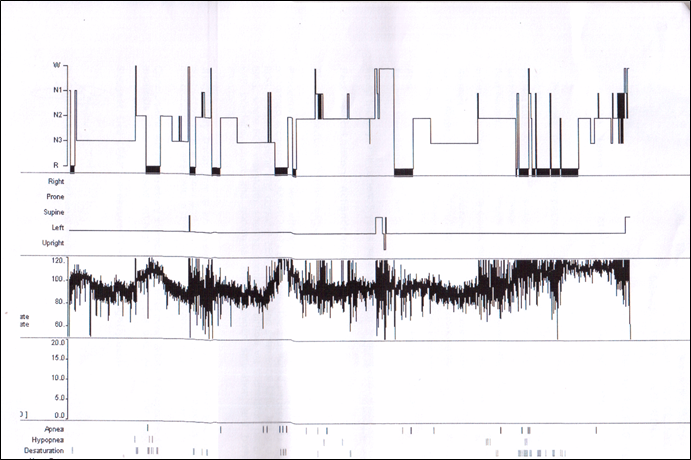
A 9 years old female child with achondroplasia had frequent episodes of difficulty in breathing and cyanosis usually early morning since the age of 2 ½ years. She was admitted many times with each episode requiring intubation and mechanical ventilation. X-Ray chest showed mild prominence of pulmonary conus. Echocardiography showed a mildly elevated pulmonary pressure of 55mg Hg. CT cervical spine was normal. MRI of the brainstem and cervicomedullary junction showed hyperintensities in the cervical cord and focal myelitis due to narrowed foramen magnum of 11.3 mm size. X-ray of the nasopharynx showed mild adenoidal hypertrophy. The child was evaluated for possible obstructive sleep apnea by polysomnography. Night-time pCO2 was normal. Overnight diagnostic polysomnography (1) was done which was suggestive of obstructive sleep apnea (OSA). Total sleep time (TST) apnea hypopnea index (AHI) was 13 with predominantly obstructive hypopnea (71 obstructive hypopnea & 9 central apnea) with markedly frequent desaturation with minimum oxygen saturation of 50% (Figure 1). Desaturation index was 86. Overnight polysomnographic (PSG) titration study was done in which all respiratory indices improved at continuous positive airway pressure (CPAP) pressure of 12 though number of arousals were increased on high pressure. The AHI was reduced from 13 to 3.87 events/hr. Obstructive events reduced from 71 to 10. She was advised CPAP at pressure 12 on nightly basis after which there were no further episodes of cyanosis or apnea.
Figure 1: Polysomnography showing obstructive apnea, hypopnea and desaturation episodes
Upto 75% of children with achondroplasia have sleep disordered breathing consisting of obstructive apnea, central apnea or both. Obstructive apneas are associated with midface hypoplasia and reduction in nasopharyngeal space. (2) Central apnea are reported with foramen magnum stenosis & narrow cervicomedullary junction. (2,3) In our patient there were features of both obstructive and central apnoea. Since she responded to nasal CPAP, probably her predominant symptoms were due to obstructive apnea. American Academy of Pediatrics recommends that every infant with achondroplasia should be screened for cervicomedullary compression. Symptomatic patients with a narrow foramen magnum and/or hyperintensity on MRI should undergo cervicomedullary decompression. Options for obstructive sleep apnea are adenotonsillectomy, CPAP, oxygen and tracheostomy. (2,4) Close follow up is required including annual polysomnography. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Afsharpaiman S, Sillence DO, Sheikhvatan M, Ault JE, Waters K. Respiratory events & OSA in children with achondroplasia: investigation and treatment outcomes. Sleep breath. 2011 Dec; 15(4):755-61. [CrossRef]
- DelRosso LM, Gonzalez-Toledo E, Hoque R. A 3 month old achondroplastic baby with both obstructive apneas & central apneas. J Clin Sleep Med. 2013 Mar 15;9(3): 287-289. [CrossRef]
- Zucconi M, Weber G, Castronovo V, Ferini Strambi L. Sleep & upper airway obstruction in children with achondroplasia. J Pediatr. 1996; 129(5) :743-9. [CrossRef]
- Waters KA, Everett F, Sillence DO, Fagan ER, Sullivan CE. Treatment of obstructive sleep apnea in achondroplasia: evaluation of sleep, breathing, and somatosensory-evoked potentials. Am J Med Genet. 1995 Dec 4;59(4):460-6. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2018.10
|
| Cite this article as: | | Agarwal N, Taneja S, Tandon A. Obstructive Sleep Apnea in a Patient of Achondroplasia. Pediatr Oncall J. 2018;15: 22. doi: 10.7199/ped.oncall.2018.10 |
|