Vinayak Deshmukh.
Department of Pediatrics, JNMC, Wardha, Maharashtra, India.
ADDRESS FOR CORRESPONDENCE
Vinayak Deshmukh, Associate Professor of Pediatrics, Dept of Pediatrics, Staff QUARTERS, Sawangi Meghe, Wardha- 440022.
Email: deshmukhvinayak@rediffmail.com | | Abstract | | We report an 8-year-old male child with hypothyroidism and limb muscle pseudo hypertrophy i.e. Kocher-Debre-Semelaigne syndrome (KDS) which is a rare clinical presentation. It is the type of myopathy associated with severe and long standing hypothyroidism. Pseudomuscular hypertrophy is reversible with entrain treatment. | | | | Keywords | | Hypothyroidism, KDS, Kocher Debre Semelaigne syndrome, Pseudo hypertrophy, entrain. | | | | Introduction | Kocher-Debre-Semelaigne syndrome is a rare disorder causing pseudo hypertrophy of muscles due to longstanding hypothyroidism. Usual age of presentation is between 18 months to 10 years, but may manifest in neonatal period. (1) Response to the treatment is good and pseudo hypertrophy of muscles is reversible.
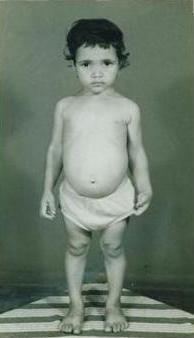
| | | | Case Report | An eight years old boy of non-consanguineous parents presented with scholastic backwardness, short stature and constipation. Mother informed us my son is dull and slow compared to his peers. On examination, he was having athletic built, coarse facies, large protruding tongue, dry mottled skin and pallor with abdominal distension. There was no evidence of malnutrition, hernia or goiter. Delayed osseous maturation was evident by open anterior fontanel. Height and weight were below third percentile. He had evidence of generalized muscular hypertrophy which was more prominent in girdle and limbs, giving an athletic appearance. (Figure 1). He could stand up from sitting position unaided. He was started on L-thyroxine at the dose of 4mcg/kg/day and he has shown marked increase in alertness with regressing muscle bulk after 4 weeks of treatment. In spite of complete regression of pseudohypertrophy, catch-up growth in the form of school performance and height was incomplete as observed after 6 months of OPD follow up. Investigations showed hemoglobin of 8.5 gm%, leucocyte count of 6500/cu mm (polymorphs 70%, lymphocytes 30%). Thyroid function tests showed Total T3 <40 ng/dl (normal 70-200 ng/dl), total T4 <1 mcg /dl (normal 5.5-13.5 mcg/dl), TSH >95 mIU/ml (normal 0.2-5.0 mIU/ml), which confirmed the diagnosis of hypothyroidism. Ultrasound studies for thyroid were not done. After six weeks of treatment; T3, T4 and TSH estimation was done which was normal.
Figure 1: Photograph of the patient shows generalized pseudo hypertrophy of the muscles which is more prominent in girdle and calf muscles.

 | | | | Discussion | | Kocher-Debre-Semelaigne syndrome involves muscles of extremities, limb girdle, trunk, hands and feet but it is more prominent in muscles of limbs; hence the athletic or Herculean look. (1) Pseudo hypertrophy of muscles comprised 18.7% of cases with a 2:1 female to male ratio, and it was found in various forms of hypothyroidism. Thyroid dysgenesis was the most common etiology (80.9%), (2) Calf muscles involvement is a rare clinical presentation of hypothyroidism. Its pathogenesis is unknown. Nonspecific histochemical and ultra structural changes seen on muscle biopsy return to normal with treatment. Boys are more prone. Siblings of consanguineous marriage affected children are more prone for pseudo hypertrophy of calf muscles. They usually have hypothyroidism of longer duration and severity. (3) Kocher-Debre-Semelaigne syndrome with presence of pericardial effusion an unusual presentation has been reported. The response to thyroxin replacement was excellent, with resolution of the pericardial effusion and clinical improvement. (4). Similar improvement was seen in our patient. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Tullu MS, Udgirkar VS, Muranjan MN, Sathe SA, Kamat JR. Kocher-Debre- Semelaigne syndrome: hypothyroidism with muscle pseudo hypertrophy. Indian J Pediatr 2003; 70:671-3. [CrossRef]
- Unachak K, Dejkhamron P. Primary congenital hypothyroidism: clinical characteristics and etiological study. J Med Assoc Thai. 2004 Jun; 87(6): 612-7. [PubMed]
- Nelson Text book of Pediatrics. Behraman RE, Kliegman RM & Jenson HB, eds, WB Saunders Company, Philadelphia, pp: 1875-1876.
- Dharaskar P, Tullu MS, Lahiri KR, Kondekar S, Vaswani RK. Kocher-Debre-Semelaigne syndrome with pericardial effusion. Indian J Med Sciences. 2007; 61(9): 527-530. [CrossRef]
|
| Cite this article as: | | Deshmukh V. Kocher-Debre Semelaigne Syndrome. Pediatr Oncall J. 2008;5: 121. |
|