Jesmin Hossain1, Mohammad Kamrul Hassan Shabuj2.
1Department of Pediatric Cardiology, National Heart Foundation Hospital and Research Institute, Mirpur, Dhaka, Bangladesh,
2Department of Neonatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
ADDRESS FOR CORRESPONDENCE
Mohammad Kamrul Hassan Shabuj, Assistant Professor, Department of Neonatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
Email: shabuj619@yahoo.com | | Abstract | Background: Patent Ductus Arteriosus (PDA) is a common cause of neonatal morbidity. We aimed to do this meta-analysis to compare the efficacy of paracetamol/acetaminophen and ibuprofen for the closure of hemodynamically significant PDA (hsPDA) in preterm infants.
Method: Medline, Embase, Google scholar databases were searched for citations. We included 14 studies that had compared hsPDA closure in paracetamol group versus ibuprofen group in premature infants. Pooled proportion of hsPDA closures and odd’s ratio were analyzed.
Result: Pooled Odd’s ratio for intervention comparison meta-analysis was 1.20 (95% CI 0.85 to 1.70), signifying no difference of events of PDA closure in paracatamol group versus ibuprofen group and pooled proportion analysis of PDA closure with paracetamol was 77.8% (95%CI 73.76 to 81.49) in the fixed effect and 79.07% (95% 69.44 to 87.30) in random effect model . In the ibuprofen group pooled protion of PDA closure were 79% (95% CI 74.46 to 83.95) and 79.9 (95% CI 73.26 to 85.95) in fixed and random model respectively. Difference of proportion was 1.49% (95% CI, -4.65 to 7.44) (p=0.62).
Conclusison: Our study colcluded that closure of hsPDA in premature infants were comparable both in terms of intervention comparison metaanalysis and isolated proportion meta-analysis with paracetamol or ibuprofen.
| | | | Keywords | | Ibuprofen, PDA, paracetamol, Meta-Analysis | | | | Introduction | | Ductus Arteriosus (DA) is the shunt that makes communication between pulmonary artery to aorta and it is one of the basic shunts necessary in the prenatal life to maintain fetal circulation. (1,2) After birth due to transition of circulation, it closes. At 24 to 72 hours it functionally closes in the term and healthy newborns. (3,4) Ductus closure happens after birth due to higher postnatal levels of partial pressure of arterial oxygen (PaO2), increase in pulmonary flow, and decline of prostaglandin E2 (PGE2) (5 6) with decreased vasodilatory effect on DA. (7–9) It may remain open due to some unwanted effect at transition. It is reported that patent ductus arteriosus (PDA) is common amongst preterm infants. PDA is present in 30% of very low birth weight infants (< 1500 g) (10) and in 50 % of extremely low birth weight ones (< 1000 g). (11) Failure to close DA in the preterm infants for long period of time leads to severe respiratory distress syndrome (RDS), requires prolonged ventilatory support and increases chances of pulmonary hemorrhage, bronchopulmonary dysplasia (BPD), necrotizing enterocolitis (NEC), renal functional impairment, intraventricular-hemorrhage (IVH), periventricular leukomalacia (PVL), cerebral palsy, and death. (12) These aforementioned complications indicates the urgency of PDA treatment. There are several modalities of medical treatment and first choices are cyclooxygenase inhibitors indomethacin or ibuprofen. (13) But these cyclooxygenase inhibitors have several adverse effects like peripheral vasoconstriction, gastrointestinal (GI) bleeding and GI perforation, decreased platelet aggregation, hyperbilirubinemia, and renal failure. (14) acetaminophen (paracetamol) is the alternative treatment option. It acts by inhibiting the activity of prostaglandin synthase at the peroxidase enzyme. (15) Recent studies showed that paracetamol has the similar effect as cyclooxygenase inhibitors with less or no adverse effects. So we did this meta-analysis to compare the efficacy of paracetamol/acetaminophen and ibuprofen for the closure of hemodynamically significant PDA (hsPDA) in preterm infants | | | | Methodology | Data Search and data extraction
Medline, Embase, Google scholar databases were searched with predefined set criteria. We extracted the articles that included hsPDA in preterm infants. hsPDA was defined as the presence of at least one of the following criteria: internal ductal diameter 1.4 mm/kg body weight, left atrium (LA)-to-aortic (Ao) root ratio > 1.4, unrestrictive pulsatile trans ductal flow. (16) We included articles that only used paracetamol, paracetamol with placebo and paracetamol versus ibuprofen. We used the Medical Subject Heading term and Title as searching procedure of the articles. Two reviewers independently extracted data, if there was any disagreement it was solved by consensus.
Quality Assessment of the Studies
The quality of the trials, assessed by the Cochrane recommended Grading Recommendation Assessment and Evaluation (GRADE) (17) were moderate grade quality.
Statistical Analysis:
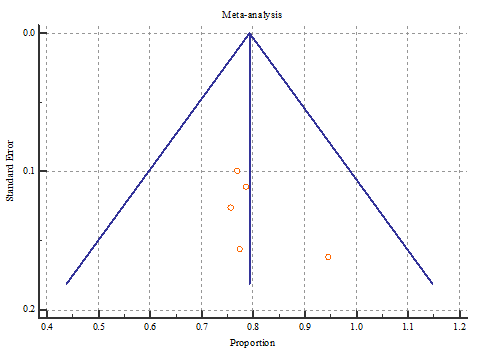
The extracted data were analyzed by the weighted Odd’s ratio by Mantel-Heinzel fixed and random effect model. Review manager (Revman, version 5.3 The Nordic Cochrane Centre, The Cochrane Collaboration, 2011; Copenhagen, Denmark), Medcalc free trial copy software were used for data analysis. The pooled data were presented by the Forest plot and heterogeneity were analyzed by Q and I2 statistics and publication bias was assessed by Funnel plot.
| | | | Results | We included 14 studies with 689 premature infants having hsPDA. Five studies were controlled trials (3 randomised controlled trials (RCT), 2 controlled trials) and included 655 ifants (Fig.1, Table 1). Those 5 studies were analyzed for pooled Odd’s ratio for intervention comparision meta–analysis and showed pooled Odd’s ratio 1.20 (95% CI 0.85 to 1.70) signififying no difference of PDA closure in paracatamol group versus ibuprofen group (Fig.2). For pooled proportion analysis, all 15 studies were included in paracetamol group (5 controlled trials and 10 case series) and 5 studies were in the ibuprofen group. Pooled proportion of PDA closure with paracetamol was 77.8% (95% CI 73.76 to 81.49) in fixed effect and 79.07% (95% CI 69.44 to 87.30) in random effect model (Fig.3) and publication bias shown by Funnel plot showed good symmetry (Fig.4). In case of ibuprofen group pooled protion of PDA closure were 79% (95% 74.46 to 83.95) and 79.9 (95% CI 73.26 to 85.95) in fixed and random model respectively (Fig.5). Difference of proportion was 1.49% (95% CI, -4.65 to 7.44) (p=0.62) and publication bias of the studies showed symmetry of the funnel plot (Fig 6).
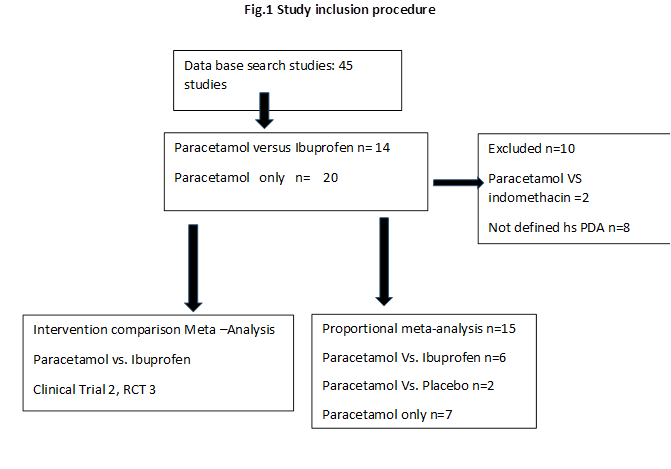
Table 1. Characteristics of the included Studies
| Authors Name and Year |
Type of Study |
Gestational age |
Route of administration |
Sample size |
PDA closure Paracetamol (n) |
PDA closure ibuprofen (n) |
Dose |
| Bagheri 2016 (18) |
RCT |
< 37 weeks |
oral |
129 (Para n=67, Ibu n=62) |
55 1st course |
47 1st course |
Para 15mg/kg 6 hourly, ibu initially 20mg/kg then 2 doses 10mg/kg for 2 days |
| Yang 2016 (19) |
RCT |
< 37 weeks |
oral |
Para n=44, Ibu n =43 |
31 |
33 |
ibu 10mg/kg then 2 doses 5mg/kg for 2 days |
| Yurttulan 2013 (20) |
Case series |
Preterm |
oral |
Only para n=6 |
5 |
- |
Para 15 mg/kg every 6 h for 3 d |
| Dang 2013 (21) |
RCT |
< 34 weeks |
oral |
Para n=80, Ibu n =80 |
65 |
63 |
para 15 mg/kg 6 h for 3 days
ibu 10mg/kg then 2 doses 5mg/kg for 2 days |
| Oncel 2014 (22) |
RCT |
< 30 weeks |
oral |
90 |
29/40 1st course |
31/40 1st course |
para 15 mg/kg 6 h X 3 days
ibu 10mg/kg then 2 doses 5mg/kg for 2 days |
| Nadir E 2014 (23) |
Case series |
24-27 weeks |
oral |
7 |
5 |
- |
para 15 mg/kg 6 h x 7 days |
| Harkin 2016 (24) |
Placebo controlled trial |
< 32 weeks |
IV |
48 |
20/23 |
- |
20 mg/kg within 24 hours of birth, followed by 7.5 mg/kg 6 hrly for 4 days |
| El Mashad 2017 (25) |
RCT |
< 28 weeks |
IV |
Para n =100, ibu n=100 |
80 1st course |
80 1st course |
15 mg/kg/6 h for 3 days, ibu 10mg/kg then 2 doses 5mg/kg for 2 days |
| Desai 2012 (26) |
Case series |
- |
oral |
5 |
2 |
- |
25 mg/kg/dose, maintenance dose of 15 mg/kg/dose for 5 days |
| Hammerman 2011 (27) |
Case series |
26-32 weeks |
|
8 |
6 |
- |
15 mg/kg per dose every 6 hours 48 hours |
| Gianluca 2014 (28) |
Case series |
26 + 2 weeks |
oral |
8 |
6/8 |
- |
7.5 to 15 mg/kg every 4–6 hours maximum daily dose 60mg/kg |
| Dash (29) |
RCT |
Para 28.5 + 2.7) weeks, Indo 28.9 (+ 2.6) weeks |
oral |
77 |
36/36 |
35/37 |
Para 15 mg/kg/dose four times daily for 7 days |
| Memisoglu (30) |
Case series |
23-30 |
IV |
11 |
10 |
- |
Para 15?mg/kg every 6?h for three days |
| Sinha R (31) |
Case series |
27-33 weeks |
oral |
10 |
10 |
- |
15 mg/kg 8 hourly |
Note: RCT- randomized controlled trials, Para – Paracetamol, Indo –indomethacin, Ibu – Ibuprofen, IV- intravenous
Fig. 2: Forest Plot of Patent Ductus Arteriosus (PDA) closure in paracetamol group versus ibuprofen
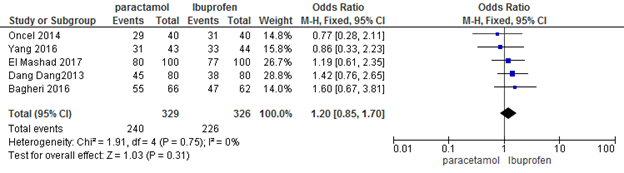
Fig.3 Forest plot for pooled proportion of patent ductus arteriosus (PDA) closure with paracetamol
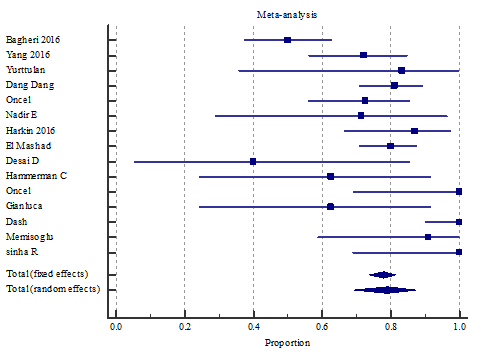
Fig.4 Funnel Plot for publication bias analysis in paracetamol group.
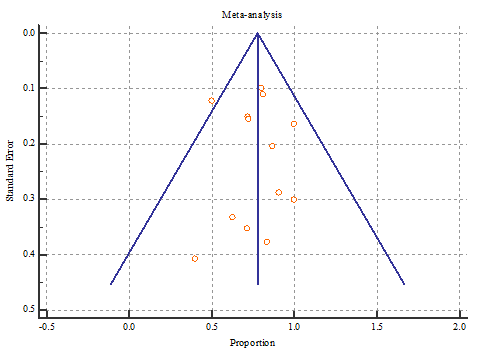
Fig. 5: Forest Plot for pooled proportion of PDA closure with Ibuprofen
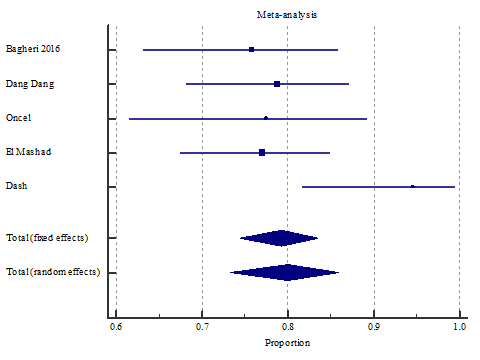
Fig.6: Funnel Plot for publication bias analysis in Ibuprofen group.
 | | | | Discussion | The first choice of treatment for PDA is primarily ibuprofen and recent studies have shown that paracetamol can be used to treat PDA in preterm infants. (32) In hsPDA, the recommended dose of paracetamol is 15mg/kg/6 hourly for 3 days and the recommended dose for ibuprofen is 10mg/kg followed by 10mg/kg for 2 days. But one study conducted by Bagheri (16) used ibuprofen 20mg/kg then 10mg/kg for 2 days and found no significant difference in closure of PDA between the two groups. In this meta-analysis we compared the efficacy of paracetamol with the efficacy of ibuprofen in term of closure of hsPDA in premature infants in five controlled trials. We had also analyzed the proportion of PDA closure in 10 case series and 5 controlled trials. Our study finding was comparable with the several studies but these studies only did the invention comparison meta-analysis with 2 RCT. (31, 33) Dash et al (31) showed the similar result (OR, 1.2 (95% CI, 0.71-2.03, P = 0.5)). Ohlsson et al (33) also showed that there was no significant difference with oral paracetamol versus oral ibuprofen treatment (typical relative risk (RR) 0.90, 95% (CI) 0.67 to 1.22; typical risk difference (RD) -0.04 (95% CI -0.16 to 0.08; I2 = 0 %) for RR and 23% for RD). Those studies also showed the comparison of the adverse effect of the both drugs. The adverse effect of ibuprofen are well established so we did not do the further comparison. The meta-analysis of the 5 randomized controlled trials (RCTs) done by Huang et al (35) showed that the efficacies for the primary (risk ratio (RR): 1.03, p = .56) and overall PDA closure were comparable between the two medications (RR: 1.02, p = .62). Our study also found that Odd’s ratio of closure and proportion of closure PDA were similar in both groups.
The strength of our study were that both proportion and intervention comparison were done. We included studies for intervention comparison which were homogenous (I2 =00). Publication bias was analyzed and showed funnel plot symmetry.
Our study had several limitations. No subgroup analysis was done for different dose schedule, for duration of treatment and for route of administration of drugs. Not all the included studies were RCT. We did not show the adverse effect comparison.
| | | | Conclusion | | Our study colcluded that closure of hsPDA in premature infants were comparable both in terms of intervention comparison meta-analysis and isolated proportion meta-analysis with paracetamol of ibuprofen. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Fanos V, Pusceddu M, Dess A, Marcialis MA. Should we definitively abandon prophylaxis for patent ductus Arteriosus in preterm new-borns? Clinics. 2011;66:2141–2149. [CrossRef] [PubMed]
- Mitra S, Florez ID, Tamayo ME, Aune D, Mbuagbaw L, Veroniki AA, et al. Effectiveness and safety of treatments used for the management of patent ductus arteriosus (PDA) in preterm infants: A protocol for a systematic review and network meta-analysis. BMJ Open 2016; 6:e011271. [CrossRef] [PubMed] [PMC free article]
- Abdel-Hady H, Nasef N, Shabaan AE, Nour I. Patent Ductus Arteriosus in Preterm Infants: Do We Have the Right Answers? BioMed Research International. 2013, Article ID 676192. https://doi.org/10.1155/2013/676192. [CrossRef]
- Benitz WE and Committee on fetus and newborn. Patent Ductus Arteriosus in Preterm Infants. Pediatrics. 2016; 137: e20153730. [CrossRef] [PubMed]
- Bhattacharya M, Asselin P, Hardy P, Guerguerian AM, Shichi H, Hou X, et al. Developmental changes in prostaglandin E2 receptor subtypes in porcine ductus arteriosus: Possible contribution in altered responsiveness to prostaglandin E2. Circulation.1999;100: 1751–1756. [CrossRef] [PubMed]
- Bouayad A, Kajino H, Waleh N, Fouron JC, Andelfinger G, Varma DR, et al. Characterization of PGE2 receptors in fetal and newborn lamb ductus Arteriosus. Am J Physiol Heart Circ Physiol. 2001;280:2342–2349. [CrossRef] [PubMed]
- Antonucci R, Bassareo P, Zaffanello M, Pusceddu M, Fanos V. Patent ductus arteriosus in the preterm infant: new insights into pathogenesis and clinical management. J Matern Fetal Neonatal Med. 2010;23:34–37. [CrossRef] [PubMed]
- Clyman RI, Mauray F, Roman C, Heymann MA, Payne B. Factors determining the loss of ductus Arteriosus responsiveness to prostaglandin E. Circulation. 1983;68:433–436. [CrossRef] [PubMed]
- Abrams SE, Walsh KP, Coker SJ, Clarkson MJ. Responses of the post-term arterial duct to oxygen, prostaglandin E2, and the nitric oxide donor, 3-morpholinosydnonimine, in lambs and their clinical implications. Heart. 1995;73:177–181. [CrossRef]
- Reller MD, Rice MJ, McDonald RW. Review of studies evaluating ductal patency in the premature infant. J Pediatr. 1993;122:S59–62. [CrossRef]
- Schmidt B, Roberts RS, Fanaroff A, Davis P, Kirpalani HM, Nwaesei C, et al. Indomethacin prophylaxis, patent ductus arteriosus, and the risk of bronchopulmonary dysplasia: further analyses from the Trial of Indomethacin Prophylaxis in Preterms (TIPP). J Pediatr. 2006;148:730–4. [CrossRef] [PubMed]
- Benitz WE. Treatment of persistent patent ductus arteriosus in preterm infants: time to accept the null hypothesis? J Perinatol. 2010;30:241–52. [CrossRef] [PubMed]
- Demirel G, Erdeve O, Dilmen U. Pharmacological Management of PDA: oral versus intravenous medications. Curr Clin Pharmacol. 2012;7:263–70. [CrossRef] [PubMed]
- Zecca E, Romagnoli C, De Carolis MP, Costa S, Marra R, De Luca D. Does Ibuprofen increase neonatal hyperbilirubinemia? Pediatrics. 2009;124: 480–4. [CrossRef] [PubMed]
- Lucas R, Warner TD, Vojnovic I, Mitchell JA. Cellular mechanisms of acetaminophen: role of cyclo-oxygenase. FASEB J. 2005;19:635–7. [CrossRef] [PubMed]
- Patrick JM, Arvind S. Towards rational management of the patent ductus arteriosus: the need for disease staging. Arch Dis Child Fetal Neonatal Ed. 2007; 92:F424–F427. [CrossRef] [PubMed] [PMC free article]
- Gopalakrishna G, Mustafa RA, Davenport C, Scholten RJ, Hyde C, Brozek J, et al. Applying Grading of Recommendations Assessment, Development and Evaluation (GRADE) to diagnostic tests was challenging but doable. J Clin Epidemiol. 2014;67:760-8. [CrossRef] [PubMed]
- Bagheri MM, Niknafs P, Sabsevari F, Torabi MH, Bahman Bijari B, Noroozi E et al. Comparison of Oral Acetaminophen Versus Ibuprofen in Premature Infants With Patent Ductus Arteriosus. Iran J Pediatr. 2016; 26: e3975. [CrossRef] [PubMed] [PMC free article]
- Yang B, Gao X, Ren Y, Wang Y, Zhang Q. Oral paracetamol vs. oral ibuprofen in the treatment of symptomatic patent ductus arteriosus in premature infants: A randomized controlled trial. Exp Ther Med. 2016;12:2531-2536. [CrossRef] [PubMed]
- Yurttutan S, Oncel M, Arayici S, Uras N, Altug N, Erdeve O, Dilmen U. A different first-choice drug in the medical management of patent ductus arteriosus: oral paracetamol. J Matern Fetal Neonatal Med.2013; 26:825-827. [CrossRef] [PubMed]
- Dang D, Wang D, Zhang C, Zhou W, Zhou Q, Wu H. Comparison of oral paracetamol versus ibuprofen in premature infants with patent ductus arteriosus: A randomized controlled trial. PLoS ONE. 2013;8: e77888. [CrossRef] [PubMed] [PMC free article]
- Oncel M, Yurttutan S, Erdeve O, Uras N, Altug N, Oguz S, et al. Oral paracetamol versus oral ibuprofen in the management of patent ductus arteriosus in preterm infants: A randomized controlled trial. J Pediatr. 2014; 164:510-4e1.
- Nadir E, Kassem E, Foldi S, Hochberg A, Feldman M. Paracetamol treatment of patent ductus arteriosus in preterm infants. J Perinatol. 2014;34: 1-2. [CrossRef] [PubMed]
- Härkin P, Härmä A, Aikio O, Valkama M, Leskinen M, Saarela T, Hallman M. Paracetamol Accelerates Closure of the Ductus Arteriosus after Premature Birth: A Randomized Trial. J Pediatr. 2016;177:72-77. [CrossRef] [PubMed]
- El-Mashad A, El-Mahdy H, El Amrousy D, Elgendy M. Comparative study of the efficacy and safety of paracetamol, ibuprofen, and indomethacin in closure of patent ductus arteriosus in preterm neonates. Eur J Pediatr. 2017; 176:233-240. [CrossRef] [PubMed]
- Dasai D, Kluckow M. The efficacy of paracetamol for PDA closure in preterm infants. J Paediatr Child Health. 2012; 48: 126-127.
- Hammerman C, Bin-Nun A, Markovitch E, Schimmel M, et al. Ductal Closure With Paracetamol: A Surprising New Approach to Patent Ductus Arteriosus Treatment. Pediatrics. 2011;128:e1618-e1621. [CrossRef] [PubMed]
- Terrin G, Conte F, Scipione A, Bacchio E, Conti MG, Ferro R, et al. Efficacy of paracetamol for the treatment of patent ductus arteriosus in preterm neonates. Ital J Pediatr. 2014; 40:21. [CrossRef] [PubMed]
- Dash SK, Kabra NS, Avasthi BS, Sharma SR, Padhi P, Ahmed J. Enteral paracetamol or Intravenous Indomethacin for Closure of Patent Ductus Arteriosus in Preterm Neonates: A Randomized Controlled Trial. Indian Pediatr. 2015;52:573-578. [CrossRef] [PubMed]
- Memisoglu A, Alp Ünkar Z, Cetiner N, Akalın F, Ozdemir H, et al. Ductal closure with intravenous paracetamol: a new approach to patent ductus arteriosus treatment. J Matern Fetal Neonatal Med. 2016;29:987-990. [CrossRef] [PubMed]
- Das RR, Arora K, Naik SS. Efficacy and Safety of Paracetamol versus Ibuprofen for Treating Patent Ductus Arteriosus in Preterm Infants: A Meta‑analysis. J Clin Neonatol. 2014;3:183-190. [CrossRef]
- Lucas R, Warner TD, Vojnovic I, Mitchell JA. Cellular mechanisms of acetaminophen: role of cyclo-oxygenase. FASEB J. 2005;19(6):635–7. [CrossRef] [PubMed]
- Ohlsson A, Shah PS. Paracetamol (acetaminophen) for patent ductus arteriosus in preterm or low-birth-weight infants. Cochrane Database Syst Rev. 2015;(3):CD010061. [CrossRef]
- Huang X, Wang F, Wang K. Paracetamol versus ibuprofen for the treatment of patent ductus arteriosus in preterm neonates: a meta-analysis of randomized controlled trials. J Matern Fetal Neonatal Med. 2017, Jul 18:1-7.
DOI: https://doi.org/10.7199/ped.oncall.2018.29
|
| Cite this article as: | | Hossain J, Shabuj M K H. Paracetamol versus Ibuprofen in the Closure of Patent Ductus Arteriosus: Proportion and Intervention Comparison Meta - Analysis. Pediatr Oncall J. 2018;15: 62-68. doi: 10.7199/ped.oncall.2018.29 |
|