Tatiana Pereira1, Graça Barros Loureiro1, Ana Maria Ferreira1, Marta Guimarães2,3, Paulo Guimarães1.
1Department of Pediatrics, Centro Hospitalar de Entre o Douro e Vouga, Santa Maria da Feira, Porto, Portugal,
2Department of General Surgery, Centro Hospitalar de Entre o Douro e Vouga, Santa Maria da Feira, Porto, Portugal,
3Anatomy Department, Biomedical Sciences Institute Abel Salazar (ICBAS) University of Porto, Portugal.
ADDRESS FOR CORRESPONDENCE
Tatiana Pereira, Department of Pediatrics, Centro Hospitalar de Entre o Douro e Vouga, Rua Dr Candido Pinho 5, 4520-161 St Maria Feira, Porto, Portugal.
Email: taty.pereira.0@gmail.com | | Keywords | | Superior Mesenteric Artery Syndrome, Vomiting, Surgery | | | Superior mesenteric artery syndrome (SMAS) also known as Wilkie syndrome is a rare condition which results from an acute angulation of the superior mesenteric artery, with consequent compression of the third duodenal segment (D3), leading to chronic, intermittent or acute, complete or partial obstruction. (1,2) Approximately 15 causes of SMAS have been described, however in scoliosis repair surgery, the onset and presentation of intestinal obstruction can be acute. (3) Conservative initial treatment is recommended in all patients and is usually successful. (2)
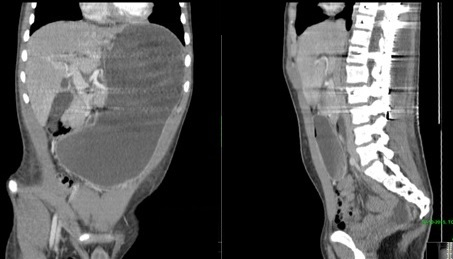
We present the case of a 16 year old adolescent boy who came to the emergency department because of vomiting (more than 10 episodes) within the previous 24 hours. He had spinal fusion surgery for correction of severe scoliosis a week ago. On physical examination, he was in pain, dehydrated and had marked abdominal distension. On auscultation there were diminished bowel sounds. Abdominal tenderness was observed mainly in the periumbilical region. Plain abdominal X-Ray revealed gastric air-fluid levels with distended stomach, and computed tomography (CT) of the abdomen and pelvis demonstrated a marked gastric and slight duodenal dilation, down to the level of D3 ( Figure 1). This raised clinical suspicion of SMA syndrome. The patient was subsequently transferred to a reference center where conservative initial treatment was initiated based on our diagnosis, with clinical success.
Figure 1: Abdomen and pelvis CT shows marked gastric and slight duodenal dilation, down to the level of D3
The differential diagnosis of acute onset of vomiting in a pediatric patient is vast. Intestinal occlusion is a potential cause, not usually first thought of in this particular population. (4) Acute and recurrent vomiting which is resistant to anti-emetic and gastric drugs, plus upper abdominal pain and dehydration may be the signs of SMAS. (5) The superior mesenteric artery (SMA) usually forms an angle of approximately 45° with the abdominal aorta. The third part of the duodenum crosses caudal to the origin of the SMA, coursing between the superior SMA and aorta. Any factor that sharply narrows the aortomesenteric angle can cause entrapment and compression of the third part of the duodenum as it passes between the SMA and aorta, resulting in SMAS. (5) Treatment consists of conservative measures such as nasogastric decompression and hyperalimentation followed by oral feeding with frequent small meals. If conservative treatment fails, surgical treatment may be considered. The outcome is excellent if the entity is diagnosed in a timely fashion and if the patient receives appropriate therapy. (5) Attention to the presentation and thorough investigation through imaging methods are of paramount importance. The same applies to a detailed present and past medical history. Our case highlights the relationship between SMA and major orthopedic surgery, as previously reported in the literature. (3,4)
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Singal R, Sahu PK, Goel M, Gupta S, Gupta R, Gupta A, et al. Superior mesenteric artery syndrome: A case report. N Am J Med Sci. 2010;2:392–394. [CrossRef] [PubMed]
- Ugras M, Bicer S, Coskun FT, Romano E, Ekci B. Superior mesenteric artery syndrome: A rare but life threatening disease. Turk J Emerg Med. 2017;17:70–72. [CrossRef] [PubMed]
- Pan CH, Tzeng ST, Chen CS, Chen PQ. Superior Mesenteric Artery Syndrome Complicating Staged Corrective Surgery for Scoliosis. J Formosan Med Assoc. 2007; 106: S37-45. [CrossRef]
- Pickering LK, Snyder JD. Gastroenteritis. In: Berhman RE, Kliegman RM, Jenson HB (eds). Nelson's textbook of pediatrics. 17th edn. Saunders. Philadelphia, PA. 2004: 1272–1276.
- Merrett ND, Wilson RB, Cosman P, Biankin AV. Superior mesenteric artery syndrome: diagnosis and treatment strategies. J Gastrointest Surg. 2009;13:287–292. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2018.40
|
| Cite this article as: | | Pereira T, Loureiro G B, Ferreira A M, Guimarães M, Guimarães P. Upper intestinal Occlusion - the Importance of Personal Medical History. Pediatr Oncall J. 2018;15: 79-80. doi: 10.7199/ped.oncall.2018.40 |
|