|
Dysphagia in an Adolescent Girl
Jiaxuan Siew, Zi Xean Khoo.
Department of Pediatrics, KK Women’s and Children’s Hospital, Singapore.
ADDRESS FOR CORRESPONDENCE
Jiaxuan Siew, Department of Pediatrics, KK Women’s and Children’s Hospital, 100 Bukit Timah Road, Singapore, SG 229899.
Email: siew.jia.xuan@singhealth.com.sg
Figure 1: Arrows indicate posterior indentation of the proximal esophagus seen on barium swallow fluoroscopy (A) and CT thorax (B and C).
Figure 1A

Figure 1B
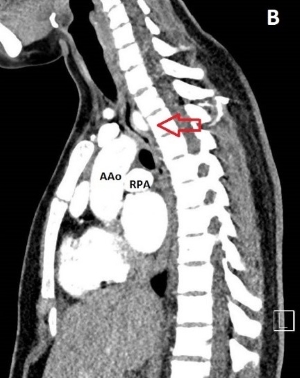
Figure 1C

|
Figure 1A

|
What is the diagnosis?
CT thorax showed an aberrant right subclavian artery (ARSA) originating as the last branch of the aortic arch, coursing posteriorly indenting the posterior esophagus, consistent with dysphagia lusoria. The patient was referred to cardiothoracic service but as her symptoms were mild, she was treated conservatively with proton pump inhibitors and lifestyle modification.
Dysphagia lusoria describes swallowing difficulties secondary to esophageal compression by an ARSA. ARSA is the most common anomaly of the aortic arch with an incidence ranging from 0.5% to 1.8%.1,2,3 While majority remain asymptomatic, symptoms may affect the very young and adults if compression is significant. Children typically present with respiratory symptoms while adult patients present with dysphagia and chest pain. Infrequently, dysphagia has been reported in pediatric patients.4,5 A barium swallow is suggestive but CT or MRI angiography are best for diagnosis.3 Surgical management is reserved for severe cases.
Contributors
JX Siew prepared the manuscript. ZX Khoo reviewed and edited the manuscript and is the primary physician of the patient.
Acknowledgments
The authors are grateful to Benjamin Wan HE for his assistance in summarizing the case. |
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
|
- Richardson JV, Doty DB, Rossi NP, Ehrenhaft JL. Operation for aortic arch anomalies. Ann Thorac Surg 1981; 31: 426–32. [CrossRef]
- Carrizo GJ, Marjani MA. Dysphagia lusoria caused by an aberrant right subclavian artery. Tex Heart Inst J 2004;31:168-171 [PubMed] [PMC free article]
- Abraham V, Mathew A, Cherian V, Chandran S, Mathew G. Aberrant subclavian artery: anatomical curiosity or clinical entity," International J Surg. 2009; 7:106–109, 2009 [CrossRef] [PubMed]
- Erami C, Charaf-Eddine A, Aggarwal A, Rivard AL, Giles HW, Nowicki MJ. Dysphagia lusoria in an infant. J Pediatr. 2013;162:1289-90 [CrossRef] [PubMed]
- Barone C, Carucci NS, Romano C. A Rare Case of Esophageal Dysphagia in Children: Aberrant Right Subclavian Artery. Case Rep Pediatr. 2016; Article ID 2539374
|
|
DOI: https://doi.org/10.7199/ped.oncall.2019.24 |
| |
Cite this article as:
Siew J, Khoo Z X. Dysphagia in an Adolescent Girl. Pediatr Oncall J. 2019;16: 60. doi: 10.7199/ped.oncall.2019.24
|