K Velmurugan, K S Kumaravel, D Satheeshkumar, S Gobinathan, P Sampathkumar.
Department of Pediatrics, Government Mohan Kumaramangalam Medical College, Salem, Tamil Nadu, India.
ADDRESS FOR CORRESPONDENCE
Dr. K S Kumaravel, MD (Pediatrics), 191A, Shankar Nagar,
Salem, Tamil Nadu 636007, India.
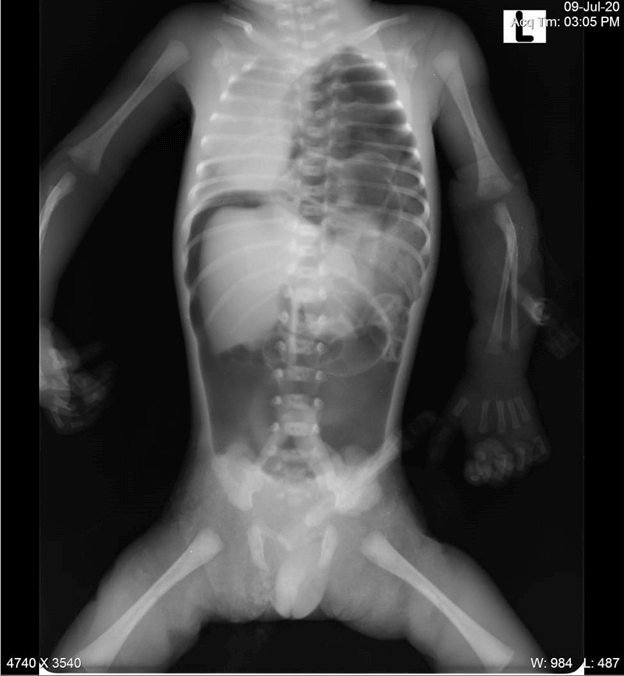
Email: kumaravelks@rediffmail.com | | Keywords | | Air leak, Preterm, Necrotizing Entero-Colitis, Mechanical Ventilation | | | A preterm male neonate was born at 31 weeks of gestation by normal delivery to a 21 years old primiparous mother. He had a birth weight of 1.3 kg. The second-trimester ultrasound scan in the mother had revealed polyhydramnios, left-sided congenital diaphragmatic hernia with bowel and stomach in the left hemithorax and hypoplastic right and left ventricles of the heart. The baby was hypotonic at birth with poor respiratory effort. He was intubated immediately and was placed on mechanical ventilation with a FiO2 of 100%. Chest X-ray taken at 1 hour of life revealed diffuse ground-glass opacity in the right hemithorax, stomach and intestinal loops occupying the entire left hemithorax, heart pushed to the right side and a massive pneumoperitoneum (Figure 1). The left lung was severely hypoplastic and could not be visualized radiologically. Despite the mechanical ventilation, inotropes, surfactant and other supportive measures, the baby was persistently hypoxic and the clinical condition deteriorated rapidly. The neonate succumbed to refractory shock and cardiac arrest at about 2 hours of life.
Figure 1. Chest and Abdominal X-ray shows diffuse ground glass opacity in the right hemithorax, stomach and intestinal loops occupying the entire left hemithorax, heart pushed to right side and a massive pneumoperitoneum.
Neonatal pneumoperitoneum can be due to surgical and non-surgical conditions. The most common cause of pneumoperitoneum in preterm neonates is necrotizing enterocolitis (NEC).1 The other surgical causes of neonatal pneumoperitoneum are perforation of the stomach, intestine, colon and rectum.2 There are five major non-surgical causes of free air in the peritoneal cavity. These are categorized as pseudo-pneumoperitoneum (due to overdistension of hollow viscera or adventitial air shadows), thoracic (associated with mechanical ventilation or cardio-pulmonary resuscitation), abdominal (following peritoneal dialysis or endoscopic procedures), gynecological (following vaginal insufflations or examinations) and idiopathic.3
A study by Khan et al revealed NEC as the cause of pneumoperitoneum in 51% neonates and in 49% it was unrelated to NEC. Further, about 7% had no apparent cause for pneumoperitoneum.4 In a study by Karaman et al, pneumoperitoneum was found in 1–3% of infants who were mechanically ventilated.5 The pathophysiology of pneumoperitoneum in these cases could possibly be secondary to pneumomediastinum or pneumothorax with extension of free air under tension in the mediastinum along the vascular planes in the chest through the normal diaphragmatic foramina or through a retrograde path through the lymphatics of the lungs or through a congenital diaphragmatic hernia or from a pleuroperitoneal fistula.
There are also reports of cases of idiopathic pneumoperitoneum which in most cases resolved spontaneously and surgical exploration is unwarranted.6,7 In our patient, the very rapid onset of pneumoperitoneum ruled out NEC as its cause. As the parents were not willing for autopsy, pneumoperitoneum due to perforation of hollow viscera could not be completely ruled out. But the possibility of mechanical ventilation as a cause of pneumoperitoneum, in this case, is more likely as the presence of diaphragmatic hernia would have eased the passage of air from an air leak in the hypoplastic left lung to enter the peritoneal cavity directly and cause a massive pneumoperitoneum. To conclude, not all cases of pneumoperitoneum are due to the perforation of hollow viscera. Other non-surgical causes should also be considered and evaluated thoroughly. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Zerella JT, McCullough JY. Pneumoperitoneum in infants without gastrointestinal perforation. Surgery. 1981;89:163-167
- Winek TG, Mosely HS, Grout G, Luallin D. Pneumoperitoneum and its association with ruptured abdominal viscus. Arch Surg. 1988;123:709-712 [CrossRef] [PubMed]
- Madura MJ, Craig RM, Shields TW. Unusual causes of spontaneous pneumoperitoneum. Surg Gynecol Obstet. 1982;154:417-420
- Khan T, Rawat J, Ahmed I, Rashid K, Maletha M, Wakhlu A et al. Neonatal pneumoperitoneum: a critical appraisal of its causes and subsequent management from a developing country. Pediatr Surg Int. 2009;25:1093-1097 [CrossRef] [PubMed]
- Karaman A, Demirbilek S, Akın M, Gürünlüoğlu K, İrşi C. Does pneumoperitoneum always require laparotomy? Report of six cases and review of the literature. [published correction appears in Pediatr Surg Int. 2006;22:303]. Pediatr Surg Int. 2005;21:819-824 [CrossRef] [PubMed]
- He TZ, Xu C, Ji Y, Sun XY, Liu M. Idiopathic neonatal pneumoperitoneum with favorable outcome: A case report and review. World J Gastroenterol. 2015;21:6417-21 [CrossRef] [PubMed] [PMC free article]
- Agrawal D, Taneja S, Avasthi S. Spontaneous Idiopathic Pneumoperitoneum in a Newborn. Pediatr Oncall J. 2012;9:16-17 [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2020.38
|
| Cite this article as: | | Velmurugan K, Kumaravel K S, Satheeshkumar D, Gobinathan S, Sampathkumar P. Pneumoperitoneum in a neonate with congenital diaphragmatic hernia. Pediatr Oncall J. 2020;17: 94-95. doi: 10.7199/ped.oncall.2020.38 |
|