Jatin Mistri, Ankur Patel, Ravi Parikh, Anuj Grover.
Department of Neonatology, Setu Newborn Care Centre, Ahmedabad, Gujarat, India.
ADDRESS FOR CORRESPONDENCE
Dr. Jatin Mistri, Setu newborn care centre, A-308, Shivalik Yash complex, Near Ankur cross road, Naranpura, Ahmedabad. 380013.
Email: jatinped@gmail.com | | Keywords | | esophageal perforation, extreme preterm | | | Esophageal perforation (EP) in neonates especially in premature neonates is a rare but potentially fatal complication with mortality rates estimated to be as high as 28%.1 Various etiological modalities have been reported to have caused EP including gastric tube insertion, endotracheal intubation, oesophageal dilation and respiratory suction catheters.1 We report a case of an extremely premature newborn that was diagnosed to have an EP.
A male newborn with a birth weight of 700 grams born at 26 weeks of gestation age was intubated and ventilated soon after birth. Routine X-ray chest was performed to check endotracheal tube position which showed abnormal course of nasogastric (NG) tube and going towards right side (Figure 1). Baby also developed right sided pneumothorax very soon which was drained with intercostal drainage tube. A repeat X-ray chest was performed with water soluble contrast on clinical suspicion of oesophageal perforation which suggested presence of esophageal leak (Figure 2). Baby was managed conservatively with total parenteral nutrition (TPN), intravenous (IV) antibiotics and was started on enteral nutrition on day 5. Once baby established full enteral feeds, a repeat oesophagogram was performed on day 14 which showed resolution of leak (Figure 3). Baby was successfully discharged on 65th day of life.
Elkof et al first reported traumatic perforations of the pharyngo-oesophageal region in the newborn.2 Since then, it has been increasingly mentioned as a possible complication. The overall estimated incidence of iatrogenic EP is 0.8% in preterm infants.3 Neonatal EP is usually iatrogenic and often due to multiple intubation attempts, oropharyngeal suctioning, nasogastric or orogastric tube insertion. Commonly patients with oesophageal perforations may present with subcutaneous emphysema and signs of respiratory distress including tachycardia, tachypnea and grunting.1
Figure 1. A. x-ray showing abnormal course of OG tube.
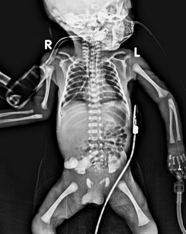
Figure 2. Water soluble contrast leaked into mediastinum.

Figure 3. Contrast study after 14 days suggestive of complete recovery.

Regarding diagnosis, chest X-ray may be used as an initial test; however, plain films maybe normal in 12% to 33% of cases.4 An unusual course of the nasogastric tube, pneumothorax, pleural effusion, subcutaneous emphysema, pneumopericardium, and pneumomediastinum have been observed on radiographs.1 Confirmative diagnosis can be made with water-soluble contrast study performed expeditiously when there is reasonable suspicion. Endoscopy has been used for diagnosis however it is not advocated for diagnosis due to other risks involved.5
Historically, management of EP was operative, but trends have shifted toward non-operative treatment. The majority of children with EP can be managed successfully by conservative measures and pleural drainage, with surgical procedures reserved for large disruptions of the esophagus, intra-abdominal perforations, and cases that fail to respond to appropriate conservative measures.6 Hodgson et al reported outcome of eleven neonates with EP and they reported that all neonates were managed with bowel rest and intravenous antibiotics for a median of 7 days; and only two patients required operative intervention.7
In conclusion, EP is not uncommon in premature infants. Early suspicion and diagnosis of EP is important because appropriate treatment usually ensures a good outcome. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Gander JW, Berdon WE, Cowles RA. Iatrogenic esophageal perforation in children. Pediatr Surg Int. 2009 May;25(5):395-401. doi: 10.1007/s00383-009-2362-6. Epub 2009 Apr 21. [CrossRef] [PubMed]
- Cairns PA, McClure BG, Halliday HL, Mc Reid M. Unusual site for oesophageal perforation in an extremely low birth weight infant. Eur J Pediatr. 1999 Feb;158(2):152-3. [CrossRef] [PubMed]
- Filippi L, Pezzati M, Poggi C. Use of polyvinyl feeding tubes and iatrogenic pharyngo-oesophageal perforation in very-low-birthweight infants. Acta Paediatr. 2005 Dec;94(12):1825-8. [CrossRef] [PubMed]
- Han SY, McElvein RB, Aldrete JS. Perforation of the esophagus: Correlation of site and cause with plain film findings. Am J Roentgenol 1985;145:537. [CrossRef] [PubMed]
- Garey CL, Laituri CA, Kaye AJ, Ostie D J, Synder C L, Esophageal perforation in children: A review of one institution's experience. J Surg Res. 2010; 164(1):13-17 [CrossRef] [PubMed]
- Panieri E, Millar AJ, Rode H, Brown RA, Cywes S. Iatrogenic esophageal perforation in children: patterns of injury, presentation, management, and outcome. J Pediatr Surg. 1996 Jul;31(7):890-5. [CrossRef]
- Hodgson K, Togo A, Moore AM, Moody A, King SK, Zani A. Neonatal oesophageal perforation: The role for non-operative management. J Paediatr Child Health. 2018 Aug;54(8):872-874. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2021.18
|
| Cite this article as: | | Mistri J, Patel A, Parikh R, Grover A. Accidental Esophageal Perforation in an extremely premature neonate. Pediatr Oncall J. 2021;18: 59-60. doi: 10.7199/ped.oncall.2021.18 |
|