Joseph Israeli1, Jennifer Ristic1, Lawrence Christie Wang2, Mauricio Restrepo3, Barbara Minkowitz1.
1Department of Orthopedics, Morristown Medical Center, Goryeb Children’s Hospital, Atlantic Health Systems, Morristown, NJ, USA,
2Department of Radiology, Morristown Medical Center, Atlantic Health Systems, Morristown, NJ, USA,
3Department of Pediatrics, Saint Clare’s Hospital, Saint Clare’s Health, Dover and Denville, NJ, USA.
ADDRESS FOR CORRESPONDENCE
Barbara Minkowitz, 261 James St., Suite 3C, Morristown, NJ, USA 07960.
Email: barbara.minkowitz@atlantichealth.org | | Keywords | | adolescent pregnancy, hip pain | | | A healthy 14.5-year-old girl presented to the orthopedist accompanied by her older sister with a chief complaint of “right hip pain” for more than one year on and off after playing softball. She had iliac apophyseal avulsion fracture one year ago which was treated with rest. The patient pointed to the right iliac crest when asked to localize pain. Physical examination revealed a 160 pound, 5 feet 4 inches tall female in no acute distress with full range of motion in bilateral lower extremities and bony tenderness over the right ilium. No changes in skin color, temperature, or swelling were noted. The hamstrings, Achilles, iliotibial band, gluteus, and hip flexor groups were all tight with passive stretching. AP and oblique lateral view pelvis radiographs (Figure 1A, B) were obtained which revealed that the prior iliac avulsion had healed, and no new bony abnormalities were noted. The patient’s pain was attributed to tendon tightness and she was given a prescription for physical therapy. The following day, radiographs were reviewed by a pediatric musculoskeletal radiologist who informed the orthopedist that her 14.5-year-old patient was “quite pregnant.” Shockingly, a fetus estimated at 28 weeks of gestation with head engaged was identified on the radiographs. The spine and long bones were visible and are outlined in Figures 2A and 2B.
Figure 1A and B. Anterior-posterior and oblique views of the pelvis show portions of a fetal skeleton compatible with a 28-week pregnancy with visualization of a head, multiple vertebral bodies, multiple ribs, and upper and lower extremities.
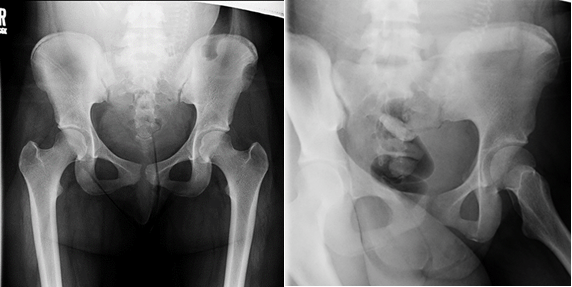
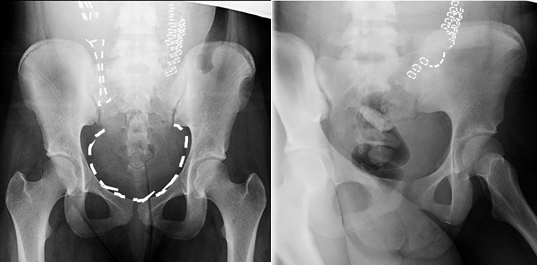
Figure 2A: Anterior-posterior and 2B. oblique views of the pelvis show portions of a fetal skeleton compatible with a 28-week pregnancy with visualization of a head, multiple vertebral bodies, multiple ribs, and upper and lower extremities. The findings are drawn onto the radiographs.
The patient had stated her last menstrual period occurred two weeks prior to the date of her office visit, and this was documented by the radiograph technologist before imaging was obtained. This was the first time that a situation like this arose in this established orthopedic practice and the patient’s pediatrician was immediately contacted. He had the patient come to his office, and she arrived accompanied by her older sister. The patient was informed of her pregnancy by the pediatrician and vehemently denied it as a possibility. After further discussion, she denied sexual abuse and admitted to known pregnancy which she denied initially due to fear. She lives with her father and older sister and said that she could not tell either of them, because she could not bring a child into her father’s house. The pediatrician sent her to the gynecologist for appropriate pre-natal care and a 28-week fetus was confirmed using ultrasound. The patient delivered a full-term healthy female in an uncomplicated vaginal birth. The hip pain resolved subsequent to childbirth. Both child and mother are well, and the mother has begun a birth control regimen. The mother plans to raise the child with the help of her family.
Adolescent hip pain could have a musculoskeletal etiology or could be gastrointestinal, genitourinary, rheumatologic, infectious, or neoplastic. A differential diagnosis for adolescent hip pain is shown in Table 1, though this is not all inclusive.1,2
Table 1. Differential diagnosis of adolescent hip pain.
| Intra-articular |
Labrum tear, femoral acetabular impingement, infection, transient synovitis, slipped capital femoral epiphysis |
| Extra-articular musculoskeletal |
Muscle sprain, bursitis, lumbar spine etiology, fracture, SI joint pain, apophysitis and apophyseal avulsion injuries, snapping hip |
| Non-musculoskeletal |
GI (appendicitis), GU, sports hernia, infection, neoplasm, inflammatory/rheumatologic, referred pain from intraabdominal, pelvic pathology, and low back problems |
In hindsight, the patient denied pregnancy prior to her radiographs and the fetus was not seen by the orthopedist. Her complaints of hip pain were due to stretching and pulling of scar tissue from the prior injury as the fetus developed. This case illustrates the importance of considering a wide differential diagnosis and avoiding tunnel vision in consideration of pediatric hip pain. In a case like this where the adolescent either denies or does not divulge pregnancy, it is important to note that radiographs during pregnancy do not increase the risk of miscarriage or cause problems such as birth defects or physical/mental developmental problems in the baby. However, they may cause a very small increased risk of the baby developing childhood cancer. For this reason, they should be avoided if possible.3
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Common Causes of Hip Pain in Children Pediatrics Clerkship | The University of Chicago. Available from URL: https://pedclerk.bsd.uchicago.edu/page/common-causes-hip-pain-children. Accessed on 21st January 2021
- Houghton KM. Review for the generalist: evaluation of pediatric hip pain. Pediatr Rheumatol Online J. 2009 May 18;7:10. [CrossRef] [PubMed] [PMC free article]
- Can I Have an X-Ray If I'm Pregnant? [Internet]. NHS Choices, NHS, Available from URL: https://www.nhs.uk/common-health-questions/pregnancy/can-i-have-an-x-ray-if-i-am-pregnant/ Accessed on 21st January 2021
DOI: https://doi.org/10.7199/ped.oncall.2021.19
|
| Cite this article as: | | Israeli J, Ristic J, Wang L C, Restrepo M, Minkowitz B. A Surprise Diagnosis at the Pediatric Orthopedic Office. Pediatr Oncall J. 2021;18: 61-62. doi: 10.7199/ped.oncall.2021.19 |
|