Shalu Gupta, S. Basu, Ashok Kumar, B. D. Bhatia.
Division of Neonatology,Department of Pediatrics, Institute of Medical Sciences, Banaras Hindu University, Varanasi, India.
ADDRESS FOR CORRESPONDENCE
Dr. Shalu Gupta, Lecturer, Dept of Pediatrics, I.M.S., Banaras Hindu University, Varanasi.
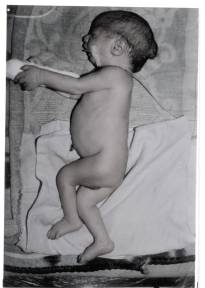
Email: drshalugupta@yahoo.co.in | | Abstract | | Meckel Gruber syndrome is a rare autosomal disorder characterized by encephalocele, polycystic kidneys, and polydactyly. The diagnosis is possible antenatally. We report a case of Meckel Gruber syndrome with a recurrence of cranium bifidum. We also found an associated posterior lingual cyst. This association is not reported earlier. | | | | Introduction | | Meckel Gruber syndrome (MGS) is a rare autosomal disorder characterized by a triad of encephalocele, polycystic dysplastic kidneys and postaxial polydactyl. It is associated with various other developmental aberrations, which make it incompatible with life. Those who survive usually suffer from severe mental retardation and neurological deficit. Prenatal diagnosis may be possible by a sonographic delineation of either the encephalocele, or the dysplastic enlarged kidneys during the first trimester and elevated alpha feto protein level, however antenatal sonography forms the cornerstone for the diagnosis. We report a case of Meckel Gruber syndrome with posterior lingual cyst. | | | | Keywords | | Encephalocele, Lingual cyst, Meckel Gruber syndrome | | | | Case Report | A full term baby born of non-consanguineous marriage was delivered through meconium-stained amniotic fluid by spontaneous vaginal delivery to 35 year old gravida 3 para one mother who also had with oligohydramnios. Mother had one spontaneous mid trimester abortion ten years back, which had a similar occipital swelling. The other sibling is a six-year-old female child, alive and healthy. She did not receive any antenatal care and there was no history of exposure to any known teratogen. On examination of the baby following congenital anomalies were noted: solitary occipital encephalocele, micrognathia, retrognathia (Figure-1), microglossia, posterior cleft palate, solitary lingual cyst (1x1 cm) from the left border of dorsal surface of posterior 1/3 rd tongue, postaxial polydactyly in all the four limbs, and bilateral palpable renal masses. Transillumination of the sac indicated presence of neural tissue. During hospital stay, baby had respiratory distress along with recurrent attacks of cyanosis. The baby was nursed in prone position with I.V. antibiotics and fluid. Orogastric feeding was gradually built up and after one week of hospital stay baby was discharged on request of the parents. On investigation, complete blood count and liver function tests were normal. Blood urea nitrogen was 72.25mg/dL and serum creatinine was 2.5 mg/dL. Ultrasonography of abdomen was suggestive of bilateral polycystic dysplastic kidneys. Ultrasonography of skull showed hydrocephalous with occipital encephalocele. Karyotyping of baby & the parents were normal. Baby was lost to follow-up.
Fig 1: Photograph showing occipital Encephalocele
 | | | | Discussion | In 1684, Mr. Christopher Krahe described a monstrous child born in Denmark, suggestive of Meckel-Gruber Syndrome (Dysencephalia splanchnocystica) (1). Moreover, Meckel first described Meckel-Gruber Syndrome in 1822, then by Gruber and later by, Opitz and Howe (2). Classically Meckel-Gruber Syndrome has been described as a congenital disorder with a triad of occipital encephalocele, polycystic dysplasia of Kidneys and polydactyly (usually postaxial). Other inconstant features include facial clefts, microcephaly, cerebellar and cerebral hypoplasia, hydrocephalous, sloping forehead, congenital heart disease, pulmonary hypoplasia (3), short limb dwarfism (4), and GI tract anomalies (5). Although fibrosis of liver has been reported in this syndrome, it is not a constant feature (6).
We report here a classical case of Meckel-Gruber syndrome with a lingual cyst. On searching literature, no case has been reported having this association. Encephalocele results from the defective closure of rostral neuropore during the fourth week of intra uterine life. However, cysts in the tongue may be derived from remnants of the thyroglossal duct. Normally the thyroglossal duct atrophies and disappears, but a remnant of it may persist and form a cyst in the tongue (7). These developmental aberrations occur early in fetal life and involves defect primarily of prechordal mesoderm. The pattern of inheritance is autosomal recessive. This syndrome is thought to be incompatible with life and results in death in early infancy; however there have been reports of survival beyond this period (8). These children usually suffer from severe mental retardation and other motor deficits.
Meckel-Gruber syndrome may be evaluated and diagnosed by sonography at the 11th to 14th weeks (9). Later in the pregnancy, oligohydramnios makes it more difficult to establish the diagnosis. Therefore antenatal diagnosis is an important part of evaluation. Couples who have had an encephalocele in the previous baby should have successive pregnancies monitored, including determination of alpha feto protein levels and ultrasound examination during first trimester. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Kompanje EJ. Features described and illustrated in 1684 suggesting Meckel-Gruber syndrome. Pediatr Dev Pathol 2003; 6(6):595-598. [CrossRef] [PubMed]
- Opitz JM and Howe JJ. The Meckel syndrome (dysencephalia splanchocystica, the Gruber syndrome). Birth Defects 1969;5:167.
- Fraser FC, Lytwyn A. Spectrum of anomalies in the Meckel syndrome. Am J Med Genet. 1981;6: 694-696.
- Malguria N,Merchant SA, Kiran KV, Verghese SL.Meckel Gruber syndrome associated with short limb dwarfism. J Postgrad Med 1996; 42(2):55-56. [PubMed]
- Ergus AT, Tas F, Yildiz E et al. Meckel-Gruber syndrome associated with gastro-Intestinal tractus anomaly. Turk J Peditr 2004;46 (4):388-392.
- Desiva MVC, Senanayake HM. Fibrosis of liver in Meckel-Gruber syndrome. Ind Pediatr 2001;38 :1325-1326.
- Urao M, Teetelbaum DH, Miyano T : Lingual thyroglossal duct cyst: A unique surgical approach. J Pediatr Surg 1996; 31 :1574. [CrossRef]
- Gazioghe N, Vural M, Seckin MS et al. Meckel-Gruber syndrome. Childs Nerv system 1998; 14(3):142-135. [CrossRef] [PubMed]
- Mittermayer C, Lee A, Brugger PC. Prenatal diagnosis of the Meckel-Gruber syndrome from the 11 th to 20 th gestational week. Ultraschall Med 2004;25(4):275-279. [CrossRef] [PubMed]
|
| Cite this article as: | | Gupta S, Basu S, Kumar A, Bhatia B D. Meckel-Gruber Syndrome with Lingual Cyst. Pediatr Oncall J. 2007;4: 17. |
|