|
T-cell lymphoblastic lymphoma: an imaging finding
Diana H. Silva1, Inês F. Ferreira1, Cristina Pedrosa1, Ana Lacerda2.
1Serviço de Pediatria, Centro Hospitalar de Setúbal, EPE, Setúbal, Portugal,
2Serviço de Oncologia Pediátrica, Instituto Português de Oncologia de Lisboa Francisco Gentil (IPOFG-Lisboa), Lisboa, Portugal.
ADDRESS FOR CORRESPONDENCE
Diana H. Silva, Rua Camilo Castelo Branco, Aptd. 140, 2910-446 Setúbal, Portugal.
Email: dianahdasilva@gmail.com
Teenager, Chest radiography, Imaging findings, T-cell lymphoblastic lymphoma, non-Hodgkin lymphoma.
Cough and thoracalgia are frequent symptoms in the Pediatric Emergency Department (PED). Although commonly linked to infections or trauma, the pediatrician must stay alert to other possible causes.
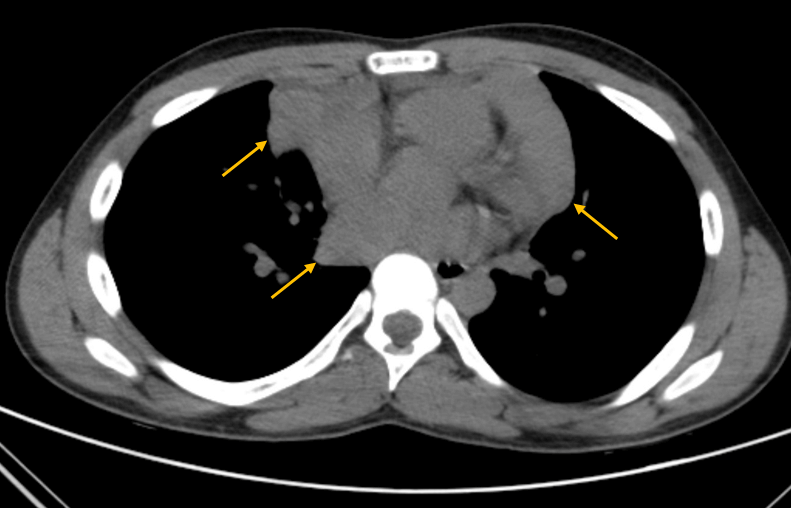
A 14-year-old boy, with a previous history of allergic rhinitis, presented to the PED due to sudden onset of a left cervical swelling. He had a six-month history of dry cough and for the last three days he had also been complaining of dyspnoea and thoracalgia (sudden onset during sleep), which was worsening and now radiating to the right shoulder. No other signs or symptoms. On examination, there was a mass on the anterior left cervical triangle, with approximately 2x3 cm, fixed to the muscle below, firm and non-tender. Laboratory studies revealed normal hemogram (hemoglobin 14.8 g/dL, leucocytes 9.3x1^3uL, neutrophils 68.2%, lymphocytes 21.6%) and elevated C-reactive protein (3.28 mg/dL, N<0.5 mg/dL) and lactate dehydrogenase (1113 U/L, N<230 U/L). The chest x-ray showed a large mediastinal mass (Figure 1) in the middle mediastinum, with a 15.13 cm width, prompting an urgent referral to Oncology. CT scan revealed several lymphoid masses, cervical bilateral (the largest on the left, 4x3 cm) (Figure 2) and at the anterior mediastinum (8.5x5.5cm, 7.5x4cm) (Figure 3). Abdominal CT was normal.
The lymph node biopsy, executed at the Oncology Unit, confirmed a diagnosis of T-cell lymphoblastic lymphoma [96% T lymphocytes (CD3+), 0,03% B-lymphocytes (CD19+) and 0,2% NK-cells (CD56+/CD3-)]. He started chemotherapy according to the DFCI-2011 protocol, which includes treatment with vincristine, doxorubicin, PEG-asparaginase, methotrexate, 6-mercaptopurine, dexamethasone and intrathecal triple therapy (prednisolone, methotrexate and cytarabine). After the induction cycle, remission was documented by CT scan. He remained under chemotherapy for two years (a total of 35 chemotherapy cycles). A CT scan performed 1 year after treatment conclusion confirmed a continued complete remission.
Figure 1. Chest x-ray: mediastinal mass (15.1 cm largest width).
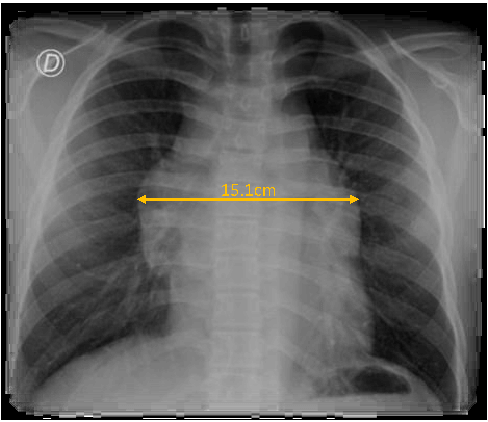
Figure 2. Cervical CT scan: left cervical lymphoid masses (the largest on the left, 4x3 cm).
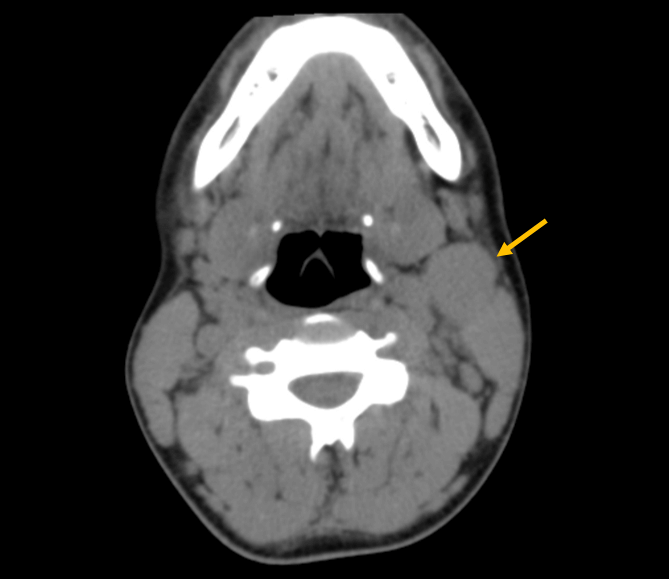
Figure 3. Thorax CT scan: multiple mediastinal lymphoid masses (8.5x5.5 cm, 7.5x4 cm).
|
What is the diagnosis?
Lymphomas are one of the most common pediatric cancers, with non-Hodgkin lymphoma accounting for about 7% the cases. T-cell lymphoblastic lymphoma is the second most common subtype of non-Hodgkin lymphoma, affecting mostly boys. Incidence is similar across all pediatric age groups, with a median age of 12 years.1 Early diagnosis remains challenging, mainly due to the wide range of presenting symptoms and their lack of specificity, such as thoracalgia and cough.2 In our case the investigation was prompted by an abnormal chest radiography and confirmed by a pathological and flow-cytometry examination.
Clinical manifestations do not tend to correlate with staging.3 Age above 10-years and T-cell phenotype are high-risk factors, associated with worse outcomes.1,4 Nonetheless, early diagnosis and risk-adapted treatment remain key to success in cancer treatment.5 |