Pankaj Venkatrao Deshpande.
Consultant Pediatric Nephrologist, Hinduja hospital, Mahim, Mumbai, India.
ADDRESS FOR CORRESPONDENCE
Pankaj Venkatrao Deshpande, A1, Candida, Plot 51 A, Sector 9 A, Vashi 400703, Maharashtra.
Email: drpankajdeshpande@gmail.com. | | Abstract | Most guidelines, including a recent review suggest blood, urine tests, an ultrasound scan of the kidneys and a renal angiogram if required in children presenting with hypertension. A dmsa scan is recommended if the ultrasound scan shows abnormal kidney/s or there is a history of urine infections.
Two boys aged 14 years and 16 years were diagnosed with hypertension. The work-up for hypertension included blood tests, urine tests, ultrasound scan of the kidneys and a renal angiogram that were all normal. A dmsa (dimercaptosuccinic acid scan) in both boys showed reduced uptake in both kidneys. In the absence of history of urine infections, these represented dysplastic changes.
These cases highlight that in children presenting with unexplained hypertension even in the absence of an abnormal ultrasound or history of urine infections, only a dmsa scan will show abnormal uptake indicating dysplastic changes despite normal renal function and absence of significant proteinuria. | | | | Keywords | Hypertension, dmsa scan, Renal dysplasia, Scarring.
| | | | Introduction | | The prevalence of hypertension in children is increasing all over the world and it presently affects at least 5% of children.1 Children having the blood pressure above the 95th centile for age are considered to have hypertension. As opposed to adults, there is likely to be a secondary cause in most children. Renovascular causes or renal parenchymal disease accounts for 60-70% of cases with pediatric hypertension.2 In most suggested guidelines for investigations in children with unexplained hypertension, a dimercaptosuccinic acid (DMSA) scan is advised only under special circumstances. The following 2 cases suggest that a dmsa scan should be part of the investigation profile for children with normal ultrasound scans also. | | | | Case Report | Case 1:
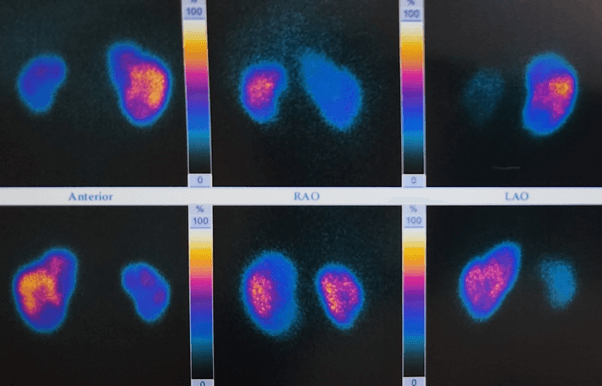
A 14-year-old boy presented with a persisting headache for a few weeks. There was no significant past history. His father had been diagnosed to have essential hypertension at 40 years of age and was on treatment. His weight was 60 kg (75th centile) and height was 160 cm (25th to 50th centile). There was no history of urine infections in the past. On examination, his blood pressure was 160/100 mm of Hg and remained high later. Systemic examination was normal and his peripheral pulses were well felt. He was started on amlodipine at 0.2 mg/kg per day. Investigations showed a normal complete blood count, a normal serum creatinine [0.8 mg/dl, estimated GFR (glomerular filteration rate) 88 ml/min], normal fasting sugar, normal lipid profile, normal urine examination and a normal urine protein/creatinine ratio (0.25 mg/mg). Complement levels (C3, C4), anti-nuclear antibodies (ANA), anti dsDNA (double stranded DNA) and ANCA (anti-nuclear cytoplasmic antibodies) and thyroid function tests were normal. An ultrasound scan with Doppler studies showed normal kidneys and bladder. Urine VMA (vanillylmandelic acid) was normal. Echocardiography showed a normal heart and eye examination was also normal. CT (computerised tomography) angiography for renal artery stenosis was normal. A dmsa scan was done that showed a reduced uptake at the upper pole of the left kidney with an inhomogeneous uptake in the right kidney that looked smaller and showed reduced uptake at upper and lower poles. The differential function was reported as 27% in the right kidney and 73% in the left kidney (Figure 1). The medication was changed to losartan (angiotensin receptor blocker) at a dose of 100 mg daily and he remains well with normal blood pressure, normal kidney function and no proteinuria at 5 years after diagnosis. A recent ultrasound scan showed the right kidney (7.7 cm X 3.8 cm) in length to be smaller than the left (9.3 X 5.4 cm).
Figure 1. DMSA scan in case 1 showing reduced uptake in both kidneys with 27% function in right kidney and 73% in left kidney.
Case 2:
A 16-year-old boy presented with vague complaints of feeling uneasy for the past few weeks. There was no history of urine infections in the past. There was no other significant past or family history. His weight was 68 kg (75th centile) and a height was 168 cm (25th centile). On examination his blood pressure was 170/90 mm of Hg and remained high. The peripheral pulses were well felt and systemic examination was normal. He was started on amlodipine at 0.2 mg/kg per day and later Telmisartan had to be added as the blood pressure remained high. The complete blood count, liver function tests, renal function, (serum creatinine 0.7 mg/dl, eGFR 90 ml/min) fasting blood sugar, lipid profile, urine examination including a urine protein/creatinine ratio (0.18 mg/mg) was normal. Complement levels (C3, C4), anti-nuclear antibodies (ANA), anti dsDNA (double stranded DNA) and ANCA (anti-nuclear cytoplasmic antibodies) and thyroid function tests were normal. An ultrasound scan of the kidneys and bladder including Doppler studies were normal. Urine VMA was normal. Echocardiography and eye examination was normal. CT angiography for renal artery stenosis was normal. A dmsa scan was done that showed impaired uptake throughout the cortex in the left kidney and inhomogeneous uptake of radiotracer in the right kidney with a cortical defect at the upper pole in the right kidney. The differential function revealed 42% function in the left kidney and 58% in the right kidney. He is currently on Telmisartan 40 mg twice a day and amlodipine has been stopped. Two years into follow-up, his blood pressure, renal function and urine protein/creatinine ratio remains normal.
| | | | Discussion | Hypertension in children is defined as the blood pressure persistently elevated above the 95th centile for age. Untreated hypertension can cause several problems, the major ones being chronic kidney disease and cerebro-vascular accidents. The prevalence of hypertension in children is increasing in recent times.1 Hypertension in children usually has a secondary cause and renal scarring has been shown to be associated with the development of hypertension in many studies. In a study that assessed the risk of hypertension in children with vesico-ureteric reflux (VUR), in a median follow-up of 72 months, renal damage was present in 48% (318/664 patients) of the patients. The probability of hypertension at 21 years was estimated to be 15% in patients with unilateral renal damage and 45% in patients with bilateral renal damage.3 However, this explains the risk of hypertension in children who are followed up for VUR or urine infections.
In a statement regarding evaluation and management of hypertension, the authors suggested a basic work-up for children with unexplained hypertension that included an ultrasound scan of the kidneys apart from blood, urine tests, eye examination and heart examination.4 A dmsa scan and MCUG (micturiting cystourethrogram) were recommended if there was suspicion of reflux nephropathy. Thus if the history did not suggest urine infections and the ultrasound scan showed normal kidneys, it was unlikely that a dmsa scan would be requested.
Both children were severely hypertensive but did not have any history of urine infections or urinary symptoms in the past. More importantly, a basic ultrasound scan of the kidneys showed normal kidneys and serum creatinine and urine protein creatinine ratio was normal. One would not suspect conditions like reflux nephropathy in such children.
Several studies have pointed out that an ultrasound scan is an inappropriate study for diagnosing renal scars in children irrespective of the grade of VUR.5,6 Thus a dmsa scan remains a gold standard for diagnosing renal scars.7,8 Again these studies were looking at children being followed up after urine infections having VUR.
A recent update about pediatric hypertension that looked at the American guidelines suggested that children aged 6 years and above did not routinely need extensive investigations if there was a positive family history, they were overweight and/or history and examination did not suggest a secondary cause.9 The aim was to suggest investigations for renovascular hypertension when indicated like in the presence of discrepant sizes of the kidneys, hypokalemia or significant hypertension. Nuclear renogram for renovascular hypertension was not recommended.
In both our cases, CT angiography was normal with no evidence of renal artery stenosis. A dmsa scan was done in both children. It was abnormal in both suggesting reduced uptake in both kidneys. In a large study retrospectively looking at the role of dmsa scan in pediatric hypertension, it was shown that 21% of the children had an abnormal dmsa.10 In most of these children, the ultrasound scan had been normal with the ultrasound revealing a very low sensitivity of only 36% in picking abnormalities. The authors labelled the abnormal dmsa findings as scarring in the kidneys suggesting that undiagnosed urine infections could be responsible for these abnormalities. They did speculate that the abnormalities could be due to scars in the prenatal period causing hypodysplasia also.
The dmsa scan in our patients showed diffuse reduced uptake in both kidneys suggesting dysplastic areas in the kidneys and are likely to be present from the prenatal period or from birth. Irrespective of urine infections or vesico-urteric reflux, the dmsa scan will be abnormal in such cases.
While a nuclear renogram is no longer the investigation of choice for detecting renal artery stenosis, in a practical sense if one starts ACE inhibitors in patients presenting like our patients and gets a dmsa scan a few weeks later, it would serve the dual purpose of identifying dysplastic areas by reduced uptake in the kidneys and also would suggest renal artery stenosis if one sees very poor function in one of the kidneys!
ACE (Angiotensin converting enzyme) inhibitors or ARBs (angiotensin receptor blockers) are the primary choice agents in treating hypertension secondary to scarring or renal dysplasia so that one can prevent hyperfiltration injury and proteinuria. These children will need close monitoring of the renal function and proteinuria as the degree of dysplasia would dictate the ultimate outcome with regards to kidney function. Our patients are presently normotensive on medications with a normal renal function and no proteinuria. It is interesting to note that in case 1, the right kidney is now appearing smaller on ultrasound 5 years later, but was normal in size and shape at presentation.
In conclusion, hypertension may be a presenting feature for children with renal dysplasia but they are likely to have a normal renal function, a normal urine protein creatinine ratio, a normal ultrasound scan and no history of urine infections. Unless a dmsa scan is advised, appropriate diagnosis of dysplasia cannot be made in these children. If the dmsa scan is done a few weeks after starting ACE inhibitors, it would also serve the dual purpose of shedding some light on the presence of renal artery stenosis. These children need close monitoring of renal function and proteinuria.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Sorof JM, Lai D, Poffenbarger T et al. Overweight, ethnicity and the prevalence of hypertension in school-aged children. Pediatrics 2004;113:475-482. [CrossRef] [PubMed]
- Arar MY, Hogg RJ, Arant BS Jr et al. Etiology of sustained hypertension in children in southwestern United States. Pediatr Nephrol (1994);8:186-189. [CrossRef] [PubMed]
- Simoese Silva AC, Silva JM, Diniz JS et al. Risk of hypertension in primary vesicoureteral reflux. Pediatr Nephrol (2007);22:459-462. [CrossRef] [PubMed]
- Bagga A, Jain R, Vijaykumar M et al. Evaluation and management of hypertension. Indian Pediatr 2007; (44)2:103-121.
- Moorthy I, Wheat D, Gordon I. Ultrasonography in the evaluation of renal scarring using DMSA scan as the gold standard. Pediatr Nephrol 2004:19:153-156. [CrossRef] [PubMed]
- Temiz Y, Tarcan T, Onol F et al. The efficacy of Tc99m dimercaptosuccinic acid (Tc-DMSA) scintigraphy and ultrasonography in detecting renal scars in children with primary vesicoureteral reflux (VUR). Int Urol Nephrol 2006; 38:149-152 21. [CrossRef] [PubMed]
- Bhatnagar V, Mitra DK, Agarwala S et al. The role of DMSA scans in evaluation of the correlation between urinary tract infection, vesicoureteric reflux, and renal scarring. Pediatr Surg Int 2002;18:128-134. [CrossRef] [PubMed]
- Rushton HG, Majd M, Jantausch B et al. Renal scarring following reflux and nonreflux pyelonephritis in children: evaluation with 99mtechnetium-dimercaptosuccinic acid scintigraphy. J Urol 1992;147:1327-1332. [CrossRef] [PubMed]
- Sinha R, Saha A, Samuels J. American Academy of Pediatrics Clinical Practice Guidelines for Screening and Management of High Blood Pressure in Children and Adolescents: What is new? Indian Pediatr 2019;56:317-321. [CrossRef] [PubMed]
- Ahmed M, Eggleston D, Kapur G et al. Dimercaptosuccinic acid (DMSA) renal scan in the evaluation of hypertension in children. Pediatr Nephrol 2008;(23):435-438. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2025.44
|
| Cite this article as: | | Deshpande P V. Dimercaptosuccinic acid (DMSA) scan in unexplained pediatric hypertension with normal ultrasound and renal angiogram. Pediatr Oncall J. 2025;22. doi: 10.7199/ped.oncall.2025.44 |
|