Sofia Poço Miranda, Inês Eiras, Cátia Juliana Silva, André Costa e Silva, Inês Correia Magalhães, Hugo Rodrigues.
Pediatrics Department, Unidade Local de Saúde do Alto Minho, Santa Luzia Hospital, Viana do Castelo, Portugal.
ADDRESS FOR CORRESPONDENCE
Sofia Poço Miranda, Unidade Local de Saúde do Alto Minho, Estrada de Santa Luzia 4904-858 Viana Do Castelo, Portugal.
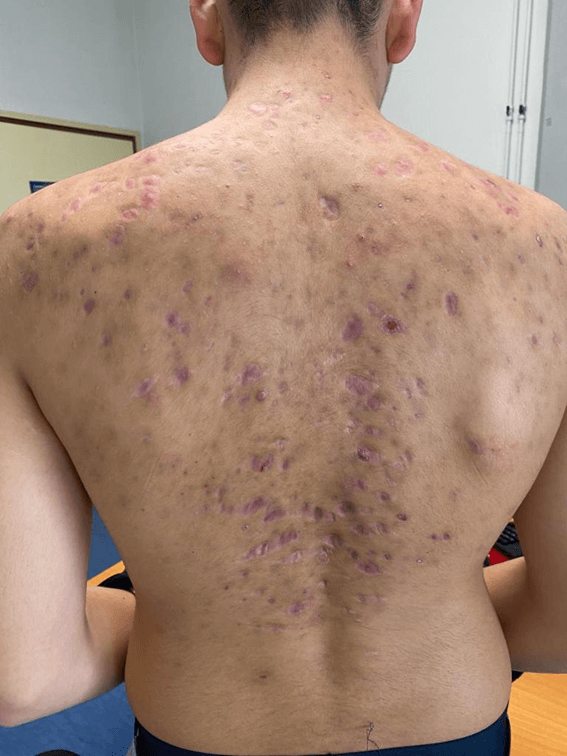
Email: sofiapocomiranda@gmail.com | | Abstract | | A previously healthy 15-year-old male adolescent was evaluated in a Dermatology consultation for inflammatory lesions, with pustules and inflammatory nodules, affecting the trunk and face, compatible with severe acne, for one year, having started treatment with oral isotretinoin. After the beginning of treatment, the lesions worsened, with the appearance of painful exuberant inflammatory lesions with purulent and bloody exudate and erosive areas, associated with myalgias of the lower limbs. Treatment was discontinued and oral prednisolone was started. After starting corticosteroids, he showed clear clinical improvement, with fewer inflammatory and exudative lesions. After 40 days of treatment, while continuing treatment with prednisolone, he presented a marked improvement in acne, so he started oral isotretinoin, with a sustained improvement in his acne, with scarring predominating and no inflammatory lesions. | | | | Keywords | | Acne vulgaris, Acne Fulminans, isotretinoin. | | | | Case Report | A previously healthy 15-year-old male adolescent was evaluated in a Dermatology consultation for inflammatory lesions, with pustules and inflammatory nodules, affecting the trunk and face, compatible with severe acne, for one year, having started treatment with oral isotretinoin. After the beginning of treatment, the lesions worsened, with the appearance of painful exuberant inflammatory lesions with purulent and bloody exudate and erosive areas, associated with myalgias of the lower limbs. No history of fever, osteoarticular pain, or other complaints were referred. The patient was referred to a new Dermatology consultation 2 months later and oral minocycline and topical mupirocin were added to the treatment. On objective examination, he was apyretic and hemodynamically stable, with a good general state with ruddy and hydrated skin and mucous membranes, with painful eruptions of inflammatory nodules, ulcers and crusts with purulent and bloody exudate, as well as extensive erosive areas, mainly on the back, pre-sternal region and face (Figure 1 and 2). Analytically, he presented hemoglobin 12.6 g/dL, leukocytosis (15,700/uL), with neutrophilia and AST, ALT, CK and DHL within normal limits. Treatment with isotretinoin and minocycline was discontinued and oral prednisolone was started. After starting corticosteroids, he showed clear clinical improvement, with fewer inflammatory and exudative lesions. After 40 days of treatment, while continuing treatment with prednisolone, he presented a marked improvement in acne, so he started oral isotretinoin. After 3 months, he showed a sustained improvement in his acne, with scarring predominating and no inflammatory lesions (Figure 3).
Figure 1. Inflammatory lesions in the dorsal region.

Figure 2. Inflammatory lesions on the face.
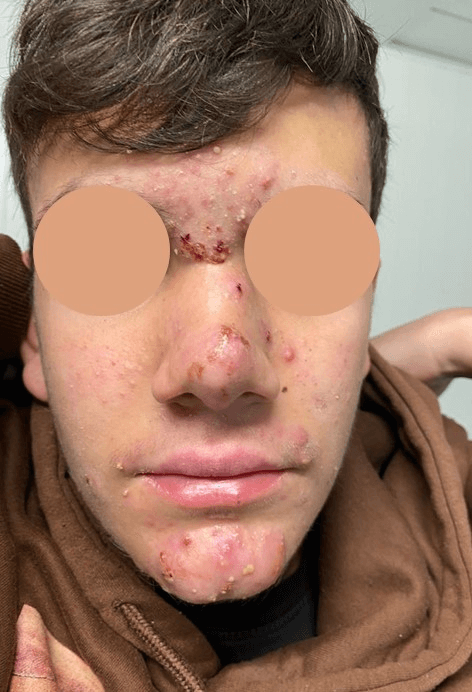
Figure 3. After three months of treatment.
| | | | Discussion | Although extremely prevalent and mostly mild, acne vulgaris can have a severe presentation. Acne fulminans or acne maligna is a rare skin disorder, characterized by its sudden appearance as an acute, painful, ulcerating and hemorrhagic clinical form of acne.1 In addition to the characteristic lesions, it may also be associated with systemic symptoms, such as fever, shivering, bone pain and arthralgias.1
Its etiology is not fully established. Acne fulminans may be triggered by the use of high doses of isotretinoin when initiating treatment in patients with severe acne.1,2 It is suggested in the literature that isotretinoin stimulates the inflammatory reaction in the skin in the early stages of treatment.3 Also, high levels of testosterone may play an important role.1 The genetic component also has a contribution in the etiology of acne fulminans, however, the pattern of heritability is not known.1 Acne fulminans may be part of the synovitis, acne, pustulosis, hyperostosis and osteitis syndrome (SAPHO), pyogenic arthritis, pyoderma gangrenosum and acne syndrome (PAPA), pyoderma gangrenosum, acne and hidradenitis suppurativa syndrome (PASH) and pyogenic arthritis, pyoderma gangrenosum, acne and hidradenitis suppurativa syndrome (PAPASH).1
Less than 200 cases have been described in the literature, with a predominance in male gender, between 13 and 22 years of age.1,2,4 Most cases have a prior history of acne1, typically as the presence of mild to moderate acne for 2 years or so before the development of acne fulminans.5
Acne fulminans generally has a very sudden onset1, with the appearance of hemorrhagic ulcerative lesions involving the back, chest and face, which are is pathognomonic for AF.6 When left untreated, progression to systemic involvement occurs, including systemic findings such as fever, leukocytosis, anemia, hepatosplenomegaly, myalgia and arthralgia.6 The painful ulcerative and nodular lesions crust and heal, leaving severe scarring.2 Often there is a history of previous treatment with systemic antibiotics with no sense of improvement. It has a presentation similar to acne conglobata, with numerous inflammatory nodules on the trunk, which often are painful, ulcerated, hemorrhagic and covered with crusts. Painful splenomegaly and erythema nodosum may occur associated with systemic symptoms. Inflammatory arthralgia usually affects more than one joint, typically the knees, hips and pelvis.1 In the present case, there was no history of systemic involvement.
Although according to the literature review, there are no specific laboratory changes for the diagnosis of acne fulminans7, due to the potential systemic involvement, the evaluation should include a complete blood count and evaluation of inflammatory parameters, liver function and, if there is a history of osteoarticular symptoms, imaging exams.1 Radiographs can help in evaluating if there are lytic bone lesions when osteoarticular complaints are present, with approximately 50% of cases having these radiographic findings.6 In our case only a slight leukocytosis with predominance of neutrophils was present.
Some differential diagnoses that should be considered are acne and suppurative hidradenitis (PASH) syndrome, severe cystic acne and acne conglobata, folliculitis decalvans and rosacea fulminans.1,5
The treatment of acne fulminans aims to reduce inflammation and reduce scarring.5 It includes quick initiation of high doses of oral corticosteroids to decrease the inflammatory process, in monotherapy until the lesions forms crusts and/or scabs, for usually 4 weeks, with subsequent initiation of low dose isotretinoin in association with corticoids, with slow increasing of isotretinoin dose. In this particular case, given the possible triggering role of isotretinoin, this must be suspended and only restarted after the lesions have healed, maintaining the treatment with corticoids in an initial phase, in a decreasing regime.1,2 It is necessary to maintain the treatment frequently for 3 to 4 months for optimal outcomes.2 The prognosis when appropriate treatment is instituted is usually good, with no risk of recurrence.6 In the present clinical case, we emphasize that the simultaneous treatment of isotretinoin and tetracyclines is not recommended, due to the association with the risk of intracranial hypertension of both medications.
Simultaneously with the medical treatment, the psychosocial impact of acne should not be underestimated, considering that acne can adversely affect a patient’s physical, emotional and daily life, resulting in poor self-esteem, poor body image, anxiety and depression.8
With this clinical case, the authors want to emphasize the importance of recognizing this often-underdiagnosed clinical entity. Acne vulgaris, although extremely prevalent in adolescence, with a mild to moderate presentation in most cases, may occur in severe forms with the potential for systemic involvement. Therefore, all pediatricians and primary care physicians should take this diagnosis into account, with referral to an orientation by dermatology, avoiding complications and the potential for disfiguring scars.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Zito PM, Badri T. Acne Fulminans. StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2023, StatPearls Publishing LLC.; 2023.
- Greywal T, Zaenglein AL, Baldwin HE, Bhatia N, Chernoff KA, Del Rosso JQ, et al. Evidence-based recommendations for the management of acne fulminans and its variants. Journal of the American Academy of Dermatology. 2017;77(1):109-17. [CrossRef] [PubMed]
- Fakih A, Goens J, Grozdev I, Dangoisse C, Richert B. Acne fulminans induced by a low dose isotretinoin: case report and review of the literature. Dermatol Online J. 2020;26(12). [CrossRef]
- Ashton R, Weinstein M. Acne Vulgaris in the Pediatric Patient. Pediatrics In Review. 2019;40(11):577-89. [CrossRef] [PubMed]
- McKegney CC, Schneider D. A Case of Acne Fulminans. Journal of Pediatric Health Care. 2022;36(6):603-6. [CrossRef] [PubMed] [PMC free article]
- Dessinioti C, Katsambas A. Difficult and rare forms of acne. Clinics in Dermatology. 2017;35(2):138-46. [CrossRef] [PubMed]
- Dall'Oglio F, Puglisi DF, Nasca MR, Micali G. Acne fulminans. Giornale Italiano di Dermatologia e Venereologia. 2020;155(6):711-8. [CrossRef] [PubMed]
- Hazarika N, Archana M. The psychosocial impact of acne vulgaris. Indian Journal of Dermatology. 2016;61(5):515-20. [CrossRef] [PubMed] [PMC free article]
DOI: https://doi.org/10.7199/ped.oncall.2023.52
|
| Cite this article as: | | Miranda S P, Eiras I, Silva C J, Silva A C e, Magalhães I C, Rodrigues H. When acne is not vulgar. Pediatr Oncall J. 2023;20: 143-145. doi: 10.7199/ped.oncall.2023.52 |
|