Yingna Liu1, Ronald Ikechi1,2, Christine Ramdin1, Kei U. Wong1,2.
1Rutgers New Jersey Medical School, Newark, New Jersey, USA,
2University Hospital, Newark, New Jersey, USA.
ADDRESS FOR CORRESPONDENCE
Kei Wong, Department of Emergency Medicine, Rutgers New Jersey Medical School, Medical Science Building, 185 South Orange Avenue, Newark NJ, USA 07103.
Email: kei.wong@rutgers.edu | | Abstract | | In the US, influenza activity occurs primarily through the fall and winter. However, in 2022, peak flu activity was reported in March. We hypothesized that the rates of influenza and comparable respiratory illnesses of RSV and COVID-19 in our pediatric emergency department were affected by COVID-19 pandemic-related social distancing and masking policies. We conducted a retrospective chart review from January 2017 to December 2022 for patients aged 0-18 who tested for influenza A/B, RSV or COVID-19. We used Chi-squared difference of proportions and Fischer’s exact test to evaluate differences in positive test rates three months prior and three months after lifting of a state mask mandate in May 2021 and school mask mandate in March 2022. A total of 12,851 patients tested for flu, RSV or COVID-19 from 2017 to 2022. RSV and COVID-19 positive test rates had significant differences three months prior and after lifting of both mandates (RSV p <0.0002, COVID p=0.0018). Influenza positive test rates had significant differences after lifting school mask mandates (p <0.0002). However, influenza and RSV positive test rates were significantly different between the same time periods in 2018 as compared to 2022 (influenza p <0.0002, RSV p=0.029). These results suggest that policies that reduce social distancing measures contribute to viral incidence and that virus seasonality has shifted since the COVID pandemic. Future studies may assess broader county or state data to determine whether different locations have similar outcomes after policy changes. | | | | Keywords | influenza, COVID, RSV, public health, mask mandate.
| | | | Introduction | | In the US, flu season occurs in the fall and winter. While influenza viruses spread year-round, most of the activity peaks between December and February.1 However, recent studies have shown that respiratory virus rates have increased with decreased distancing and masking measures.2,3 In March 2022, CDC reported peaking flu activity in the central and south-central parts of the United States, an unusual time for flu activity to be increasing.4 These flu infections disproportionately affect children as they bear a large disease burden and are more likely to seek medical care compared with healthy adults.5 Our goal is to examine the rates of influenza and related respiratory illnesses of RSV and COVID-19 cases seen in our pediatric emergency department and its timing related to New Jersey policy changes in social distancing and masking.6 We hope the study results may provide important data for public health engagement and planning efforts, including group outreach, timely initiation of antiviral treatment for high-risk patients and reduction in the disease burden of influenza, RSV and COVID-19 in children. | | | | Methods | | The institutional review board at Rutgers New Jersey Medical School approved this study. We conducted a retrospective chart review that included all patients aged 0-18 years old who were seen at the pediatric emergency department from January 2017 to December 2022. Patients were included if they were tested for influenza, RSV or COVID-19. Those who tested positive more than once in a two-week period were excluded. Our primary outcome was whether there was a significant difference in influenza, RSV and COVID-19 positive test rates in the 3-month period prior to as compared to after the lifting of a mask mandate in New Jersey on May 28, 2021 and lifting of a school mask mandate on March 7, 2022. Our secondary outcomes included whether there was a significant difference in influenza and RSV positive test rates in March 2018 as compared to March 2022 and the absolute number of influenza, RSV and COVID-19 positive cases in the five years. Descriptive statistics such as proportions are reported. Significant changes over time were determined with Chi-squared difference of proportions or Fischer’s exact test as applicable through Vassar Stats and Social Science Statistics online calculators, respectively. P-values were considered significant at the 0.05 confidence level. | | | | Results | A total of 12,851 patients were tested for influenza, RSV or COVID-19 from 2017 to 2022 at our site. The patients had an average age of 5.5 years (SD 4.9) with males accounting for 54.20% of those tested. The 3 months prior to the lifting of mask mandates and most social distancing policies on May 28, 2021 had significantly different positive test rates as compared to 3 months after reduction of public health measures for RSV (p < 0.0002) and COVID-19 (p=0.0018) (Table 1). However, influenza positive test rates were not significantly different (p > 0.05). The 3 months prior to lifting of school mask mandates were significantly different as compared to the 3 months after reduction of public health measures in influenza (p <0.0002), RSV (p=0.0053) and COVID-19 (p <0.0002) (Table 1). Of note, the positive test rates for influenza (p < 0.0002) and RSV (p=0.029) were significantly different in 2018 as compared to 2022 for the same time periods in March (Table 2).
Table 1. The difference in positive test rates 3 months prior compared to 3 months after policy changes. Three months after lifting of most indoor masking and social distancing on May 28, 2021, RSV and Covid-19 had positive test rates that were significantly different as compared to the prior three months. Three months after lifting of school mask mandates on March 7, 2022, RSV, Flu and Covid-19 had positive test rates that were significantly different as compared to the prior three months.
| |
3 Months Prior |
3 Months After |
|
| |
Positive Tests |
Total Tests |
Positive Tests |
Total Tests |
Significance (p) |
| May 28, 2021 |
|
|
|
|
|
| RSV |
24 |
461 |
126 |
578 |
<0.0002* |
| Flu |
0 |
461 |
1 |
578 |
>0.05 |
| Covid |
62 |
719 |
43 |
901 |
0.0018* |
| March 7, 2022 |
|
|
|
|
|
| RSV |
31 |
1173 |
14 |
1254 |
0.0053* |
| Flu |
51 |
1173 |
144 |
1254 |
<0.0002* |
| Covid |
353 |
1388 |
55 |
1452 |
<0.0002* |
Table 2. The difference in positive test rates in March 2018 as compared to March 2022 for RSV and flu. There were significant differences in both RSV and flu positive test rates between the two years.
| |
March 2018 |
March 2022 |
|
| |
Positive Tests |
Total Tests |
Positive Tests |
Total Tests |
Significance (p) |
| RSV |
34 |
168 |
5 |
62 |
0.029* |
| Flu |
147 |
522 |
7 |
107 |
<0.0002* |
Pre-COVID-19, during the 2017-2020 respiratory seasons, the occurrence of influenza began in October with peak incidence seen in January (Figure 1). The positivity rate for influenza was low (1%) in 2021 during the COVID pandemic (Table 3). After relaxation of masking and social distancing measures in May 2021, the positivity rate of influenza increased to 14% in 2022 (Table 3) and its peak incidence occurred later in May 2022 with a prolonged surge until July 2022, followed by earlier resurgence of influenza in late September-early October for the 2022-2023 respiratory season (Figure 1). Similarly, the peak incidence of RSV was detected during September 2021 in our locality, while SARS-CoV-2 had a peak incidence from October 2021 to March 2022, concurrently with cessation of public health measures (Figure 1). Of note, there has been a significant increase in viral assay testing since 2020, partly due to the development of 3-in-1 RSV-Flu-COVID PCR viral assay. However, the proportion of positive tests post-pandemic remained similar as to prior years (Table 3).
Figure 1. Absolute number of positive tests by virus.
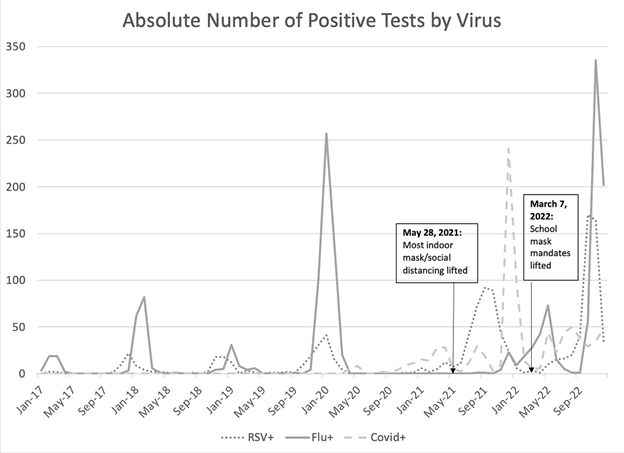
Table 3. Total tests, incidence and proportion of positive tests by virus. The total number of tests increased post-COVID pandemic, which may have been partly due to the development of 3-in-1 RSV-Flu-COVID PCR viral assay. However, the proportion positive of viruses post-pandemic were similar to prior years.
| |
2017 |
2018 |
2019 |
2020 |
2021 |
2022 |
| Influenza |
|
|
|
|
|
|
| Total tests |
337 |
755 |
575 |
1039 |
2962 |
5726 |
| Positive tests |
46 |
161 |
156 |
417 |
29 |
787 |
| Proportion+ |
14% |
21% |
27% |
40% |
1% |
14% |
| RSV |
|
|
|
|
|
|
| Total tests |
169 |
326 |
496 |
1039 |
2962 |
5726 |
| Positive tests |
36 |
56 |
80 |
62 |
407 |
481 |
| Proportion+ |
21% |
17% |
16% |
6% |
14% |
8% |
| SARS-CoV-2 |
|
|
|
|
|
|
| Total tests |
0 |
0 |
0 |
793 |
4105 |
6247 |
| Positive tests |
0 |
0 |
0 |
41 |
406 |
434 |
| Proportion+ |
0% |
0% |
0% |
5% |
10% |
7% |
| | | | Discussion | Our results suggest that viral incidence is affected by social distancing policies and public health measures, including the lifting of the May 28, 2021 indoor mask mandate and March 7, 2022 school mask mandate. The changes in influenza, RSV and COVID-19 rates were affected by lifting of mask mandates and social distancing, suggesting that public health policies can help shape the seasonality of respiratory viruses. Of note, the seasonality of the viruses has already drastically changed with the COVID-19 pandemic7,8, with influenza and RSV rates having changed in specific timeframes from 2018 as compared to 2022.
Both RSV and SARS-CoV-2 absolute positive tests began to rise shortly after the mask mandates resolution, contrary to prior RSV peak timeframes. Additionally, flu positive rates began to rise earlier than previously, starting a steep upward climb in positive rates in September 2022. These results support the preventative effects of masking and social distancing in the spreading of viruses, which may help future health policies to moderate viral spread.
However, this study was only limited to one pediatric ED and future studies may look at a broader county or the state to assess whether different locations may be affected differently by masking and social distancing policies. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- CDC - National Center for Immunization and Respiratory Diseases (NCIRD)- Flu Season.https://www.cdc.gov/flu/about/season/flu-season.htm. July 6, 2022.
- Foley DA, Yeoh DK, Minney-Smith CA, Martin AC, MaceAO, Sikazwe CT, Le H, Levy A, Moore HC, Blyth CC. The Interseasonal Resurgence of Respiratory Syncytial Virus in Australian Children Following the Reduction of Coronavirus Disease 2019-RelatedPublic Health Measures. Clin Infect Dis. 2021 Nov2;73(9):e2829-e2830. doi: 10.1093/cid/ciaa1906.PMID: 33594407; PMCID: PMC7929151. [CrossRef] [PubMed] [PMC free article]
- Osama El Assal, Anne Hall, Scott Pangonis, KaileyRemien, Ann Kennon Ulicny; The Impact of COVID-19Pandemic Social Distancing and Mask Mandates on the Prevalence of Influenza and RSV During Their Peak Season. Pediatrics February 2022; 149 (1 Meeting Abstracts February 2022): 193.
- CDC - National Center for Immunization and Respiratory Diseases (NCIRD)- Flu Activity Increasing Late in the Season. https://www.cdc.gov/flu/spotlights/2021-2022/flu-activity-increasing-late.htm. July 6, 2022.
- Grohskopf, L. A., Sokolow, L. Z., Broder, K. R.,Olsen, S. J., Karron, R. A., Jernigan, D. B., &Bresee, J. S. (2016). Prevention and control of seasonal influenza with vaccines recommendations of the Advisory Committee on Immunization Practices-United States, 2016-17 influenza season. Morbidity and Mortality Weekly Report: Recommendations and Reports, 65(5), 1-52. [CrossRef] [PubMed]
- https://covid19.nj.gov/faqs/nj-information/reopening-guidance-and-restrictions/are-schools-open-what-are-the-safety-requirements#direct-link.
- Hamid S, Winn A, Parikh R, et al. Seasonality of Respiratory Syncytial Virus - United States, 2017-2023. MMWR Morb Mortal Wkly Rep 2023;72:355-361. DOI: http://dx.doi.org/10.15585/mmwr.mm7214a1 [CrossRef] [PubMed] [PMC free article]
- Lee SS, Viboud C, Petersen E. Understanding the rebound of influenza in the post COVID-19 pandemic period holds important clues for epidemiology and control. Int J Infect Dis. 2022 Sep;122:1002-1004. doi: 10.1016/j.ijid.2022.08.002. Epub 2022 Aug 4. PMID: 35932966; PMCID: PMC9349026. [CrossRef] [PubMed] [PMC free article]
DOI: https://doi.org/10.7199/ped.oncall.2025.8
|
| Cite this article as: | | Liu Y, Ikechi R, Ramdin C, Wong K U. The Effect of COVID-19 on Influenza, RSV and COVID-19 Activity Following the Reduction of Pandemic-Related Public Health Measures. Pediatr Oncall J. 2025;22. doi: 10.7199/ped.oncall.2025.8 |
|