Andreas Chiabi1, Kate Kan1,2, Anaëlle Massom1, Cecilia Fomenky1, Samuel Angwafor1,2, Denis Nsame Nforniwe2.
1Department of Clinical Sciences, Faculty of Health Sciences, The University of Bamenda, Cameroon,
2Pediatric Service, Regional Hospital Bamenda, North West Region, Cameroon.
ADDRESS FOR CORRESPONDENCE
Andreas Chiabi, Department of Clinical Sciences, Faculty of Health Sciences, University of Bamenda, 39, Cameroon.
Email: andy_chiabi@yahoo.co.uk | | Abstract | Background: Despite the fact that efforts are being made, the mortality rates due to preventable and treatable causes still remain high in children, especially in the under-fives. The study aimed at describing the pattern, outcome of paediatric morbidities and determine factors associated with mortality at the Paediatric unit of the Bamenda Regional Hospital (BRH).
Methods: This was a retrospective study of paediatric admissions at the children’s ward of the BRH from 1st January 2016 to 31st December 2022. Children aged 3 months to 15 years admitted in that unit, within the study period were enrolled in the study.
Results: Major causes of admissions were: malaria, lower respiratory tract infections, diarrhea, and major causes of death were severe malaria, meningitis, and pneumonia. Most of the patients were discharged cured (93.1%), 0.6 % were referred, and 4.1% were discharged against medical advice. The mortality rate was 2.2% and factors associated with mortality were living in a rural setting, late presentation (>10 days after onset of symptoms), and prolonged hospital stay (> 3 weeks). The majority of the deaths (54.8%) occurred between 10 pm, and 3am, and lower rates were between 6 am, and 3 pm.
Conclusion: Malaria preventive measures and infant immunizations should be reinforced to avert common infant morbidities. | | | | Keywords | | Pediatric admissions, morbidities, mortality, outcome, Cameroon. | | | | Introduction | Child health is a fundamental human right and ill health often leads to disability, impaired activities that distort family activities as hospital admission may occur leading to increased financial burdens to governments, health systems, and parents.1 Outcome of a hospitalized ill child could be improved resulting in discharge or death increasing the burden of mortality among children and young adolescents. The World Health Organization (WHO) in 2020 reported infectious morbidities like respiratory tract infections, diarrhoeal diseases, and malaria as the leading causes of over one million deaths in older children and young adolescents; most of these diseases are preventable. These represent a potentially avoidable disease burden and the goal of ending preventable child deaths; a primary component of Sustainable Development Goal.2,3
Children and adolescent mortality remain a public health concern in developing countries.4 Globally, 85% of deaths among children and adolescents in 2018 occurred in the first five years of life, accounting for 5.3 million deaths of which infections and communicable diseases were the leading causes of childhood morbidity and mortality.5
In sub-Saharan Africa, patterns vary in different countries. In Ethiopia, the leading causes of admissions in children were community-acquired pneumonia, pulmonary tuberculosis, and asthma, with malnutrition and infections accounting for most deaths.6 In Nigeria, severe malaria, septicaemia, and pneumonia were the main causes of admissions, and septicaemia, severe malaria, and pneumonia were the most commonest causes of death, in children.7
In Cameroon, severe malaria was the most frequent cause of admissions to a referral hospital, and coma and impaired consciousness were associated with high mortality.8 This study aimed to assess the patterns of admissions, outcomes of the children, and factors associated with mortality in hospitalized children at the Bamenda Regional Hospital (BRH) in Cameroon. This will help make decisions on healthcare policies to reduce global morbidity and mortality in children.
| | | | Methods & Materials | Study design: A descriptive retrospective study conducted over 7 years from 1st January 2016 to 31st December 2022 in the paediatric unit of BRH in the Bamenda Health District (BHD), North-West Region (NWR) of Cameroon.
Selection criteria: Our study population comprised all paediatric patients who were admitted at the children’s ward of the BRH during the period of study.
All children between the ages of 3 months and 15 years admitted in this ward from 2016 to 2022, were enrolled in the study. Patients’ files with incomplete data on essential elements (age, gender, diagnosis, and outcome) were excluded from the study.
Data management and analysis: Data obtained from the hospital files of these children included age, sex, date of admission, length of hospitalization, diagnosis, and outcome of the admission. The data obtained was represented in frequency tables, charts, and graphs, with continuous data expressed in means and standard deviation. Categorical data was analyzed by Chi-square and <0.05 was considered statistically significant.
Ethical clearance: Ethical clearance was obtained from the Institutional Review Board of the Faculty of Health Sciences of the University of Bamenda (No 2023/0818H/UBa/IRB), while administrative authorization was obtained from the Northwest Regional Delegation of Public Health and the director of the Bamenda Regional Hospital. | | | | Results | A total of 8646 admissions were enrolled, and the ages of the participants ranged from 3 months to 180 months (15 years), with a mean of 55 months (4.6 years) ± 50.6 months (4.2 years). There was a male predominance (56.7%), with a sex ratio of 1.3. Majority were aged 1 to 5 years (36.0%) and resided in rural areas (53.9%) as shown in Table 1.
Table 1. Characteristics of the study population (N= 8648).
| Variables |
Number (N) |
Percentage (%) |
| Sex |
| Male |
4902 |
56.7 |
| Female |
3744 |
43.3 |
| Age |
| [3 months-1 year] |
2688 |
31.1 |
| [1-5 years] |
3116 |
36.0 |
| [5-10 years] |
1653 |
19.1 |
| [10 - 15years] |
1189 |
13.8 |
| Residence |
| Urban |
3986 |
46.1 |
| Rural |
4660 |
53.9 |
The most common causes of admission were malaria (38.0%), followed by pneumonia/ bronchopneumonia (14.7%) and gastroenteritis (12.5%) (Figure 1).
Figure 1. Main causes of admissions.
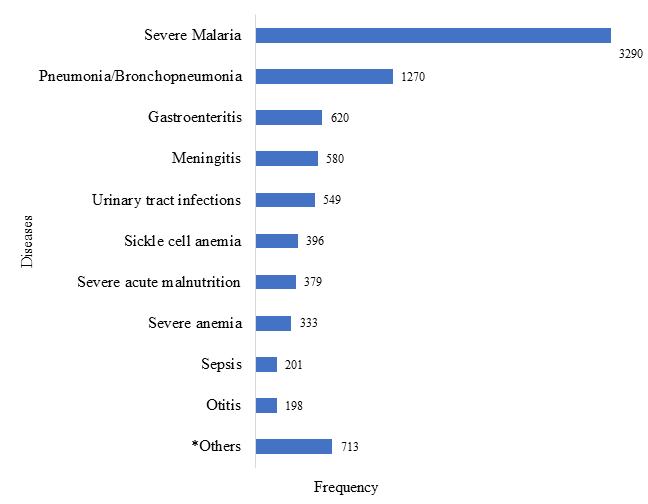
* Abscess, acute rheumatic fever, appendicitis, brain tumour, cerebral palsy, diabetes, drowning, encephalitis, epilepsy, hernia, leukaemia, lymphoma, nephrotic syndrome, trauma.
Majority of cases (93.1%) were discharged cured, and a significant proportion were discharged against medical advice (4.1%) while 2.2% died with 0.6% referrals (Table 2).
Table 2. Outcome of the admitted patients.
| Outcome |
Number (N) |
Percentage (%) |
| Treated and discharged |
8046 |
93.1 |
| DAMA* |
357 |
4.1 |
| Referred |
53 |
0.6 |
| Died |
188 |
2.2 |
| Total |
8646 |
100.0 |
* Discharged against medical advice
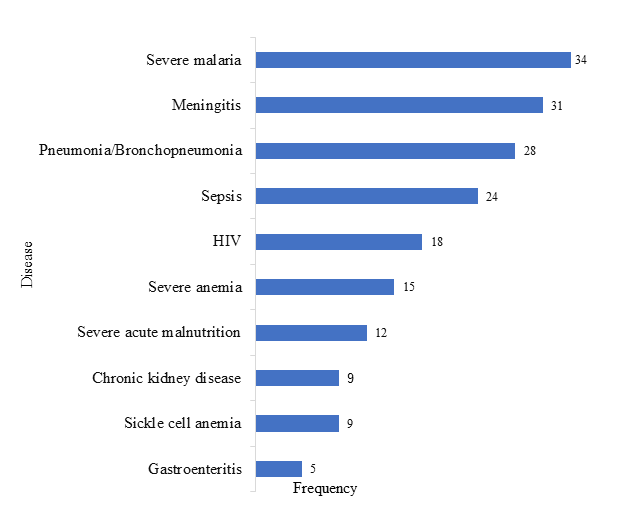
A total of 188 patients died accounting for a 2.2% mortality rate. The main causes of death were severe malaria 34 (16.5%), meningitis 31 (18.1%), and pneumonia/bronchopneumonia 28 (14.8%) as shown in Figure 2.
Figure 2. Main causes of deaths.
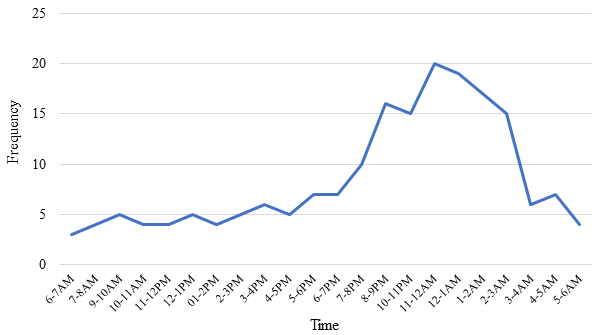
Fewer deaths (18.1%) occurred during the day, with deaths increasing from 4 pm to 9 pm, with peak mortality (54.8%) noted between 10 pm and 3 am (Figure 3).
Figure 3. Time of deaths during the day.
We observed an increased chance of death with those residing in a rural setting compared to those in urban areas (aOR=2.09; CI95% (1.52-2.86); p=0.000) as shown in Table 3.
Table 3. Association of sociodemographic status and mortality.
| Variables |
Dead |
Survive |
OR [95% CI] |
p-value |
Multivariate logistic regression |
| n |
% |
n |
% |
aOR [95% CI] |
p-value |
| Age groups |
| [3 months-1 year] |
63 |
33.5 |
2945 |
31.0 |
Reference |
|
Reference |
|
| [1-5 years] |
42 |
22.3 |
2923 |
36.3 |
0.57[0.38-0.84] |
0.05 |
0.55[0.34-0.90] |
0.18 |
| [5-10 years] |
35 |
18.6 |
1547 |
19.2 |
0.90[0.60-1.36] |
0.60 |
0.81[0.48-1.37] |
0.43 |
| [10-15 years] |
48 |
25.5 |
1083 |
13.5 |
1.76[1.20-2.57] |
0.04 |
1.27[0.76-2.13] |
0.36 |
| Sex |
| Male |
98 |
52.1 |
3748 |
43.2 |
0.83[0.62-1.12] |
0.20 |
0.88[0.61-1.28] |
0.88 |
| Female |
90 |
47.9 |
4570 |
56.8 |
Reference |
|
Reference |
|
| Residence |
| Urban |
56 |
47.9 |
4570 |
56.8 |
Reference |
|
Reference |
|
| Rural |
132 |
70.2 |
4271 |
53.1 |
2.09[1.52-2.86] |
<0.001 |
2.08[1.39-3.10] |
<0.001 |
Admission within 24 hours of the onset of symptoms reduced the risk of death (aOR=0.19; CI 95% (0.07-0.56); p=0.03). Late presentation 5 days after onset of symptoms, and more than 10 days after onset of symptoms were associated with increased risk of death (aOR=24.48; CI95% (015.96-43.95); p=0.00), and (aOR=345.87; CI95% (197.24-606.18); p=0.00) respectively, as shown in Table 4.
Table 4. Association of duration of symptoms before admission and mortality.
| Variables |
Dead |
Survive |
OR [95% CI] |
p-value |
Multivariate logistic regression |
| n |
% |
n |
% |
aOR [95% CI] |
p-value |
| <1 day |
4 |
2.1 |
3758 |
46.7 |
0.19[0.07-0.56] |
0.03 |
0.19[0.07-0.56] |
0.03 |
| [1 day-5 days] |
21 |
11.2 |
3811 |
47.4 |
Reference |
|
Reference |
|
| [5 days-10 days] |
65 |
34.6 |
427 |
5.3 |
27.63[16.72-45.64] |
<0.001 |
24.48[15.96-43.95] |
<0.001 |
| >10 days |
98 |
52.1 |
52 |
0.6 |
342.01[198.32-589.83] |
<0.001 |
345.87[197.34-606.18] |
<0.001 |
Mortality increased with prolonged hospital stay as patients who spent more than 3 weeks were more likely to die (aOR=2.58; CI95% (1.35-4.94); p=0.04) (Table 5).
Table 5. Association of duration of hospitalization and mortality.
| Variables |
Dead |
Survive |
OR [95% CI] |
p-value |
Multivariate logistic regression |
| n |
% |
n |
% |
aOR [95% CI] |
p-value |
| 1 week |
112 |
59.6 |
5093 |
68.1 |
1.56[1.01-2.39] |
0.44 |
1.20[0.71-2.02] |
0.41 |
| [1-2] weeks |
26 |
13.8 |
1840 |
22.9 |
Reference |
|
Reference |
|
| [2-3] weeks |
16 |
8.5 |
403 |
0.2 |
2.81[1.49-5.29] |
<0.01 |
3.08[1.38-6.88] |
0.06 |
| >3 weeks |
34 |
18.1 |
712 |
8.8 |
3.37[2.01-5.67] |
<0.001 |
2.58[1.35-4.94] |
0.04 |
| | | | Discussion | In this study, a total of 8646 children were admitted to the general paediatric unit of Bamenda Regional Hospital over 7 years. The majority (56.7%) of patients were males with a sex ratio of 1.3. This male predominance was observed in other studies.9, 10, 11
The vast majority (66.08%) of our study participants were aged less than 5 years which was noted in other studies.7,12
Preventable diseases remain the greatest contributors to childhood morbidity in consonance with World Health Organization.13 Severe malaria, lower respiratory tract infections, and gastroenteritis were the leading causes of hospital admissions. These findings are similar to those of other African studies.1,14
The mortality rate was 2.2%, lower than for Chiabi et al9, Koum et al8, and Lahmini et al15 who noted 4.6%, 3.98%, and 62.3% respectively.
The DAMA (discharge against medical advice), rate of this study of 4.1% was lower than 5.0% in a study by Hoque et al in India, 201216, Agbesanwa et al in Nigeria, 2023 who had 5.0%11 Our current DAMA rate may be attributed to some of the reasons given by parents which include: financial constraints, domestic obligations, inconvenience of hospitalization, perception that the child is well enough to leave the hospital and extended length of stay in the hospital.
Infectious diseases were the leading causes of mortality in our study with severe malaria, meningitis, and pneumonia ranking which corroborates with other studies in Africa8, 11, and the World Health Organization stating infectious diseases as the leading cause of childhood mortality.17 Contrary to the above studies, reported congenital diseases as the most common cause of death.15,18
We noticed a steady low level of mortality during the day from 6 am to 3 pm, increasing between 4 pm and 9 pm, and highest rates between 10 pm and 3 am. This increased rate of mortality mostly during the evening coincides with a change of nursing teams with consequently decreased attention and vigilance. The same factors with drowsiness and fatigue could explain the increase in mortality between 7 pm and 3 am.
Significant factors associated with mortality were living in a rural setting, duration of symptoms before admissions (>10 days), and duration of hospitalization (>3 weeks) were significant on multivariate analysis.
Residing in rural areas had a statistically significant association with mortality than those who resided in urban areas which is comparable to previous studies.9, 15 This could be due to difficulties in accessing health care services, and increased risk of infectious diseases due to poor sanitation.
Early (<24 hours) hospital presentation had a statistically significant association with mortality as it decreased the chances of death. Late presentation, 5 days after onset of symptoms, was associated with a higher risk of death, and much higher if the presentation was 10 days or more after onset of symptoms. This suggests that late presentation might be a contributing factor to mortality in line with Oninla et al in Nigeria, 2018 who showed that late presentations to the hospital were the leading cause of high mortalities among hospitalized children.14
Length of stay in the ward for >3 weeks had a statistically significant association with mortality than those who stayed <3 weeks. This was also noted by Pranab et al, in India12, who noted that long stays of patients were associated with increased mortality.
The main limitation of this study is its retrospective nature. The diagnoses were taken from the files and were made by the physicians who treated the children, so the exactitude could not be verified.
| | | | Conclusion | | From this study, it is observed that the major causes of admissions were malaria, lower respiratory tract infections, diarrhea, and the major causes of deaths were severe malaria, meningitis, and pneumonia. Most of these diseases are vaccine-preventable, and affect mostly children less than 5 years. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Ahmed MA, Musa IR, Mahgoub HM, Al-Nafeesah A, Al-Wutayd O, Adam I. Patterns, Outcomes and Predictors of Pediatric Medical Admissions at Gadarif Hospital in Eastern Sudan. Front Pediatr. 2022; 10(3):175-82. [CrossRef] [PubMed] [PMC free article]
- World Health Organization. Child mortality and causes of death [Internet] [WHO]; 2021 [Accessed 15 June 2023]. Available from: https://www.who.int/data/gho/data/themes/ topics/topic-details/GHO/child-mortality-and-causes-of-death.
- Reiner RC, Hay SI. The overlapping burden of the three leading causes of disability and death in sub-Saharan African children. Nat Commun. 2022;13:7457. [CrossRef] [PubMed] [PMC free article]
- Koum DK, Penda CI, Endale LM, Essome H, Moukongo CM, Foko LPK, et al. Paediatric Mortality: Aetiologies and Predictors among Children Aged 1 Month to 15 Years in a Tertiary Hospital in Douala, Cameroon. Open J Pediatr. 2021;11:360‑78. [CrossRef]
- United Nations International Children's Emergency Fund. Child mortality report 2019 [Internet]. [IGME]: [UNICEF]. [Accessed 12 Jan 2023]. Available from: https://www.unicef. org/media/60561/file/UN-IGME-child-mortality-report-2019.
- Gordon DM, Frenning S, Draper HR, Kokeb M. Prevalence and Burden of Diseases Presenting to a General Pediatrics Ward in Gondar, Ethiopia. J Trop Pediatr. 2013;59:350 57. [CrossRef] [PubMed]
- Okoronkwo NC, Onyearugha CN, Ohanenye CA. Pattern and outcomes of paediatric medical admissions at the Living Word Mission Hospital, Aba, South East Nigeria. Pan Afr Med J. 2018;30:202. [CrossRef] [PubMed] [PMC free article]
- Koum DK, Penda CI, Endale LM, Essome H, Moukongo CM, Foko LPK, et al. Paediatric mortality: Aetiologies and predictors among children aged 1 month to 15 years in a tertiary hospital in Douala, Cameroon. Open J Pediatr. 2021;11:360 78. [CrossRef]
- Chiabi A, Tchokoteu PF, Mboka F, Aly Toupouri, Mbeng Tabiojong, Sando Z. Morbidity and mortality trends in children in the East Province of Cameroon: a hospital-based experience in the Bertoua Provincial Hospital. Bull liais doc OCEAC 2002; 35(3).
- Seifu A, Eshetu O, Tafesse D, Hailu S. Admission pattern, treatment outcomes, and associated factors for children admitted to pediatric intensive care unit of Tikur Anbessa specialized hospital, 2021: a retrospective cross-sectional study. BMC Anesthesiol. 2022;22:13. [CrossRef] [PubMed] [PMC free article]
- Agbesanwa TA, Babatola AO, Fatunla OA, Ibrahim A, Aina FO, Ogundare EO, et al. Pattern of admissions and outcome in the children emergency department of a tertiary health institution in Southwestern Nigeria: A four-year review. Afr J Emerg Med. 2023;13:45‑51. [CrossRef] [PubMed] [PMC free article]
- Pranab KD, Arindam G, Sunil KH, Meghna M, Saba A, Anupama N. Morbidity Pattern With Treatment Outcome and Predictors of Mortality of Children Admitted to Pediatric Intensive Care Unit in a Peripheral Medical College in India. ProQuest. 2021; 59(8): 482-90.
- World Health Organization. Child mortality (under 5 years) [Internet]. [WHO]; 2020 [Accessed 14 June 2023]. Available from: https://www.who.int/news-room/fact-sheets/detail/levels-and-trends-in-child-under-5-mortality-in-2020.
- Oninla SO, Fadugbagbe AO, Oninla OA, Otetubi OA. Pattern of childhood morbidities and outcome of childhood admissions in a Nigerian public secondary healthcare facility. Annals Health Res. 2018;4:162‑73. [CrossRef]
- Lahmini W, Bourrous M. Mortality at the pediatric emergency unit of the Mohammed VI Teaching Hospital of Marrakech. BMC Emerg Med. 2020;20:57. [CrossRef] [PubMed] [PMC free article]
- Hoque S, Masud MAH, Nawshad UA. Admission pattern and outcome in a paediatric intensive care unit of a tertiary care paediatric hospital in Bangladesh - A two-year analysis. Nat Rev Dis Primer. 2012; 28 (1):14-9.
- World Health Organization. Child mortality and causes of death [Internet] [WHO]; 2021 [Accessed 15 June 2023]. Available from: https://www.who.int/data/gho/data/themes/topics/ topic-details/GHO/child-mortality-and-causes-of-death.
- Chukwu BF, Chinawa JM, Ikefuna AN, Emodi IJ. Pattern and outcome of paediatric medical admissions at the University of Nigeria Teaching Hospital (UNTH), Ituku-Ozalla, Enugu: a five-year retrospective review (2007 - 2011). Niger J Paediatr. 2013;40:354‑9. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2025.32
|
| Cite this article as: | | Chiabi A, Kan K, Massom A, Fomenky C, Angwafor S, Nforniwe D N. Patterns of Admissions and Outcome in the General Pediatric Unit in a Regional Hospital in Cameroon. Pediatr Oncall J. 2024 Apr 10. doi: 10.7199/ped.oncall.2025.32 |
|