André Morais1, Inês Candeias1, Carla Garcez2, Arnaldo Cerqueira2.
1Pediatrics Department, Hospital de Braga, Portugal,
2Intermediate Pediatric Care Unit, Hospital de Braga, Portugal.
ADDRESS FOR CORRESPONDENCE
André Morais, Rua de S.José, nº99 - 3ºD. 4710-436 - São Victor, Braga - Portugal.
Email: affmorais@gmail.com | | Abstract | A 7-year-old boy was brought to a pediatric appointment by his mother due to an abnormal sound coming from his son's chest, that she heard while he was sleeping, loud enough to wake her up. A left-sided pneumothorax was diagnosed. The boy was referred to the emergency department and then promptly treated. One month later, his mother noticed the return of the sound and suspected a relapse, bringing the child to the emergency immediately.
Hamman's sign is a distinct and loud sound synchronized with the heartbeat, typically observed in the precordial area. It is commonly associated with changes in body position. It’s pathognomonic for left-sided pneumothorax or pneumomediastinum. Although Hamman's sign is rarely encountered as a primary symptom, its presence is crucial for making an accurate diagnosis. Recognizing this rare clinical finding is important as it can help avoid unnecessary diagnostic tests. | | | | Keywords | | Hamman's Sign, Pneumothorax, Children, Diagnosis | | | | Introduction | Hamman’s sign was first described in 1937 by Louis Hamman1,2 and consists in a characteristic crunching, popping, crackling, or clicking chest noise that occurs in synchrony with heart sounds and varies with respiration. Like in this case, sometimes, it can be heard without a stethoscope. This rare phenomenon is very indicative of spontaneous pneumomediastinum and it’s considered pathognomonic for spontaneous left-side pneumothorax.3
This case report emphasizes the importance of physical examination in order to achieve a correct diagnosis. This rare, but described sign was the only symptom in this young patient that was perceived by his highly alert mother, who recognized this loud clicking sound coming from his son’s chest. Recognizing Hamman’s sign allowed not only the first diagnosis, but also a relapse, enabling a quick and prompt treatment. Almost ninety years after Hamman’s discovery, Hamman’s sign is still a clinical finding that can’t be underestimated. However, recent studies appear to show that in some cases the precordial clicking sounds are temporary and limited to the time period when the pneumothorax is small.4 | | | | Case Report | A previously healthy boy’s mother noticed, days before admission, the appearance of a chest noise
during his sleep. His mom described the noise like “two rocks beating each other, loudly”, that even woke her up. She also mentioned that the noise disappeared after his son changed his sleeping position (more audible when in left lateral decubitus). Beside this, he was completely asymptomatic, without chest pain, dyspnea or other respiratory symptoms.
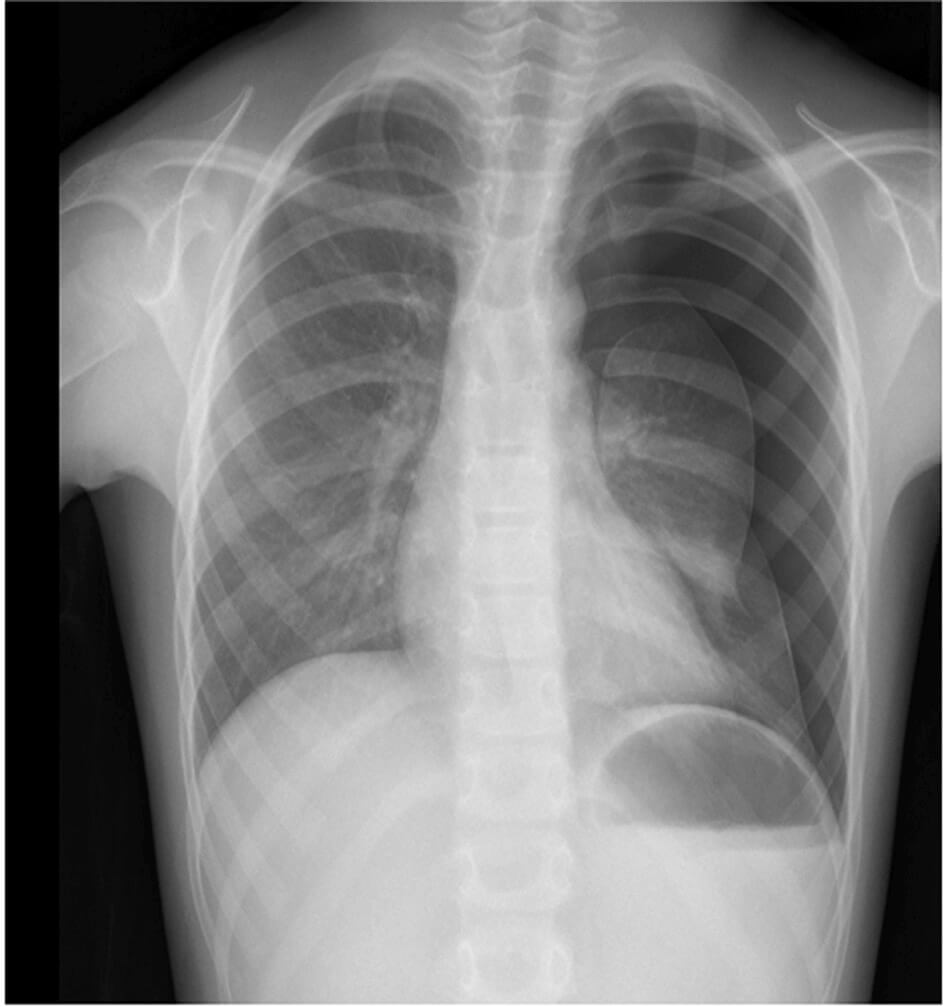
He was firstly brought to a pediatric appointment and after the presumptive diagnosis of a pneumothorax, he was referred to a level 3 hospital’s emergency department. On examination, he was hemodynamically stable, without supplemental oxygen requirement and no evidence of respiratory distress. Pulmonary auscultation showed absent breath sounds on the upper part of the left hemithorax. A simple chest radiograph and an electrocardiogram (ECG) were the first-line investigations. X-ray demonstrated a 40 mm left apical and a 22 mm lateral pneumothorax (Figure 1). Routine blood tests were also performed with normal parameters. During hospitalization, a chest computerized tomography scan was also performed, with no identification of blebs or other parenchymal/emphysematous lesions. There were never signs of pneumomediastinum. Observation and oxygen supplementation were the first measures, however, since there was no improvement, it required drainage and insertion of a chest tube. Pneumothorax persisted and a left thoracoscopic mechanical pleurodesis was needed. Remaining hospitalization was uneventful and he was discharged without any symptom or chest noise 17 days after.
Figure 1. Chest radiograph from first admission showing a large left pneumothorax.
One month later, his mom noticed the appearance of the clicking noise again, with the same characteristics, and immediately brought his son to the level 3 hospital where he was previously hospitalized. He was otherwise asymptomatic, and besides the thorax auscultation, his physical examination was unremarkable. After the relapse confirmation it was decided to repeat the previous surgical procedure and a mechanical pleurodesis was performed. During his hospitalization the boy developed a bacterial infection (Methicillin-Sensitive Staphylococcus aureus was isolated in the pleural fluid), treated with flucloxacillin in monotherapy after the MSSA isolation and a thoracoscopy with a decortication was needed. No other intercurrences were registered and he recovered completely without any sequelae. He is followed in outpatient clinic of Pediatric Pneumology without any record of complications. All the investigations were negative. Also, his mother never heard Hamman’s sign again, even during common viral respiratory infections. | | | | Discussion | Hamman’s sign is an intriguing auscultatory finding that holds diagnostic significance and should raise attention from pediatricians. Enhancing awareness of this sign and knowing in which situations it is associated can contribute to earlier diagnosis, appropriate management and improve patient outcome. Hamman’s sign is traditionally associated with the presence of pneumomediastinum and pneumothorax and its cause is yet to be discovered. General consensus is that the movement of extrapulmonary air being pulsed by ventricular contraction during the cardiac cycle is the principal cause, however others say that it may be due to free pleural air being channeled through pulmonary fissures.1,3
A thorough physical examination in pediatrics holds a vital role in the diagnostic process, particularly if there is limited access to complementary exams. The diagnosis of a small pneumothorax can be a tricky challenge, especially if the patient is asymptomatic. Nonetheless, despite the rarity of Hamman’s sign, its presence alone should immediately raise suspicion of an underlying left sided pneumothorax or a pneumomediastinum, even if our patient has no symptoms.
The treatment of a pneumothorax is still not very consensual. A stepwise approach is used depending upon the presentation and size of the pneumothorax.5,6
To the best of our knowledge, most of the described cases of Hamman’s sign in the pediatric population are associated with pneumomediastinum. In comparison to our patient, these cases usually involve slightly older individuals with the characteristic body shape of being tall and thin, which didn’t happen in this particular case. Also, our patient suffered one recurrence that was quickly recognized by his mom. Recurrent pneumothorax is the most common complication after an initial episode and could occur in about 50% of children.7
Interestingly, other reported cases emphasize the significance of modern technologies in facilitating diagnosis. In fact, it was through the use of smartphones that the diagnosis in one described case was possible. These advancements highlight the increasing role of new technologies in improving medical practices and expanding diagnostic capabilities.8
A mother plays multiple roles in the overall well-being of their children, however, the recognition of Hamman’s sign usually is not one of them. In this case, the highly alert mom recognized (twice) that something wasn’t normal and looked for help, even with his otherwise asymptomatic son, contributing to an early diagnosis.
Learning points:
► Hamman’s sign is a rare phenomenon, consisting in a characteristic crunching, popping, crackling, or clicking chest noise that occurs in synchrony with heart sounds and varies with respiration.
► Hamman’s sign is considered pathognomonic for left sided pneumothorax and pneumomediastinum.
► Despite Hamman’s sign rarity as a presenting symptom of a pneumothorax, if present, left side pneumothorax or pneumomediastinum should immediately be considered.
► An exhaustive physical examination is crucial in the diagnostic process.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Hamman L. A note on the mechanism of spontaneous pneumothorax. Ann Intern Med 1939;13:923-7. [CrossRef]
- LINTZ RM. SPONTANEOUS MEDIASTINAL EMPHYSEMA. Archives of Internal Medicine. 1943 Feb 1;71(2):256. [CrossRef]
- Remmelts HHF, Banga JD. Popping pneumothorax. The Netherlands Journal of Medicine [Internet]. 2010 Apr 1 [cited 2023 Dec 12];68(4):187. Available from: https://pubmed.ncbi.nlm.nih.gov/20421663/
- Seki K, Watanabe H, Morita R, et al. Serial Changes in Hamman's Sign Secondary to the Evolution of a Shallow Left-Sided Spontaneous Pneumothorax. Respiratory Care [Internet]. 2015 May 1 [cited 2023 May 18];60(5):e110-2. Available from: https://rc.rcjournal.com/content/60/5/e110 [CrossRef]
- Goldman RD. Spontaneous pneumothorax in children. Canadian Family Physician Medecin De Famille Canadien [Internet]. 2020 Oct 1 [cited 2023 Dec 12];66(10):737-8. Available from: https://pubmed.ncbi.nlm.nih.gov/33077450/
- Yousuf S, Cardenas S, Rezaee F. Pediatric pneumothorax: Case studies and review of current literature. Respiratory Medicine Case Reports. 2021;34(34):101548. [CrossRef]
- Seguier-Lipszyc E, Elizur A, Klin B, et al. Management of Primary Spontaneous Pneumothorax in Children. Clinical Pediatrics. 2011 Apr 11;50(9):797-802. [CrossRef]
- Thakeria P, Danda N, Gupta A, et al. Smartphone aiding in analysis of Hamman's sign. BMJ case reports [Internet]. 2019 Nov 19;12(11):e231418. Available from: https://pubmed.ncbi.nlm.nih.gov/31748357/ [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2025.64
|
| Cite this article as: | | Morais A, Candeias I, Garcez C, Cerqueira A. Highly alert mom: recognizing Hamman’s sign in children and its importance in early detection of a pneumothorax. Pediatr Oncall J. 2025;22: 85-87. doi: 10.7199/ped.oncall.2025.64 |
|