Tehsin Patel, Sruthi Nair, Prashanth RR, Anitha Haribalakrishna.
Department of Neonatology, Seth G.S. Medical College and King Edward Memorial Hospital, Mumbai, India.
ADDRESS FOR CORRESPONDENCE
Sruthi Nair, Department of Neonatology, 10th floor, MSB, KEM hospital, Parel, Mumbai 400012, India.
Email: sruthis.doc@gmail.com | | Abstract | | Congenital syphilis is a preventable infection caused by treponema pallidum usually involving multiple system. We report a case of a neonate born to mother with latent syphilis, presenting with bone changes on radiography without any clinical signs or symptoms of congenital syphilis. In this case, it is demonstrated that isolated long bone fractures can be the initial presenting sign of congenital syphilis with other classical findings possibly appearing later and early treatment for the same. We have highlighted the importance of radiological survey in asymptomatic neonates with positive serology. | | | | Keywords | | Congenital syphilis, Fracture, Metaphysitis. | | | | Introduction | Congenital syphilis (CS) is an infection caused by treponema pallidum usually involving the liver, bone and brain. Even though the disease prevalence has remained latent over the years, there has been a resurgence reported by Centre for Disease Control(CDC) in the year 2017.1,2
Among the babies born to untreated mothers, 40% are either stillborn or manifest with immediate complications like hydrops fetalis, preterm birth, low birth weight or may be asymptomatic at birth.3 Among those symptomatic, various clinical features include severe anemia, jaundice, hepatosplenomegaly, snuffles, mucocutaneous lesions, pneumonia, osteochondritis, periostitis and pseudo paralysis. These symptoms may manifest at birth or within 4 to 8 weeks of life.4
Bone involvement secondary to syphilis in neonates is an unusual presentation and those presenting as a fracture is even more rare. In a large case series reporting 60-80% of infants with CS presenting with skeletal manifestations including symmetric osteoperiostitis of long bones there were no fractures reported.5 We report a case of CS with metaphysistis of bilateral tibia and femur with left clavicular fracture and have described the importance of early identification in a resource limited setting and management for a better outcome.
| | | | Case Report | A male neonate born by vaginal delivery at 39 weeks of gestation to a 30 years old mother by spontaneous conception, with previous two uncomplicated pregnancies, with a birth weight of 3098 grams (50-90 centile) and head circumference of 35 cm (50-90 centile). Neonate required no resuscitation at birth, APGAR scores of 9 at both 1 and 5 minutes with no difficulty in extraction and was hemodynamically stable with normal physical and systemic examination including no pallor, skin lesions, hepatosplenomegaly or paucity of limb movements.
In the antenatal period, on routine evaluation, the mother was detected to be VDRL positive (Titres 1:16) and TPHA positive. She was asymptomatic and was diagnosed to have latent syphilis. She was treated with intramuscular penicillin as per CDC protocol and she was compliant with the treatment. Serological markers for HIV and HBsAg were negative. The husband also tested RPR and TPHA positive and was also treated for latent syphilis. No other family members were tested.
In the delivery room, universal precautions were followed and placental gross examination was normal and neonate was roomed with the mother in the postnatal ward and was initiated on breastfeeding. In view of the maternal history of latent syphilis, the neonate was evaluated with qualitative RPR and TPHA both of which were positive. A diagnosis of confirmed congenital syphilis was made and further evaluated and managed as per CDC guidelines.
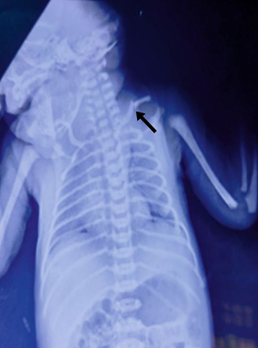
A skeletal survey done was suggestive of changes of bilateral metaphysitis with cortical thickening at diaphysis and localized destruction of the medial portion of the proximal tibial and distal femur. (Figure 1A) There was fracture of the left clavicle at the junction of medial two-thirds and lateral one-third of the bone. (Figure 1B)
Figure 1A. Radiolucency at the proximal and distal metaphysis of femur, tibia, with periosteal reaction, metaphyseal serration as shown by arrow, suggestive of congenital syphilis.
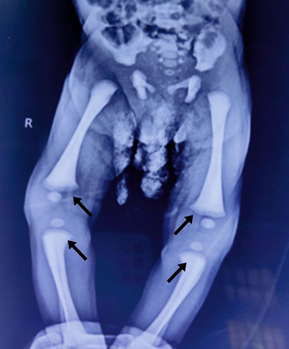
Figure 1B. Fracture of left clavicle as indicated by arrow.
Neonate was also evaluated with a hemogram, liver function test, cerebrospinal fluid (CSF) analysis, ophthalmic evaluation and neurosonogram, all of which were normal. Due to non-availability of aqueous or procaine penicillin G, Inj. ceftriaxone (75mg/kg/day OD IV and was given for 10 days).
Multidisciplinary care involving neonatologist, microbiologist, radiologist, orthopedician and clinical psychologist was provided. The fracture was managed conservatively with a figure of eight bandage and neonate was discharged on day of life 11. Family counselling regarding the need for timely follow-up was done. The repeat X-ray of long bones done on follow-up revealed resolution of bony manifestations of syphilis and fracture. Hearing assessment, neurodevelopment assessment and repeat serological testing has been planned every 2-3 monthly until the non-treponemal tests are negative. | | | | Discussion | Congenital syphilis occurs as a result of vertical transmission of treponema pallidum with the severity being determined by the stage of syphilis in the mother and the duration of fetal exposure in the uterus.6 Congenital syphilis can be diagnosed using treponemal and non-treponemal tests. However, interpretation is difficult as both maternal treponemal and non- treponemal IgG antibodies can be transferred through the placenta to the fetus. Thus, RPR and TPHA can show false positive results in uninfected infants of seropositive mothers.7 In our index case, mother was VDRL and TPHA positive and neonate was RPR and TPHA positive.
The majority of infants born to mothers with untreated syphilis appear normal and have no clinical or laboratory evidence of infection at birth, but may develop manifestations of disease months to years later if left untreated. Early congenital syphilis refers to those clinical manifestations that appear in the first 2 years of age and clinical disease that occurs after 2 years of age is designated as late congenital syphilis. The most specific sign for late congenital syphilis is Hutchinson’s triad which consists of Hutchinson’s teeth, eighth cranial nerve deafness and interstitial keratitis.6 Bone lesions in congenital syphilis mainly involve tibia and other long bones which is generally multiple and symmetrical. Cremin and Fisher in 1970, in their report of 102 cases of CS from South Africa, considered their skeletal findings not due to an active inflammation of the bones but dystrophic in nature instead.8 They classified their findings into three different groups: Group I: Metaphyseal dystrophy, Group II: Osteitis-like dystrophy and Group III: Periosteal dystrophy.9 As per this classification of Cremin and Fisher, the index neonate’s bone changes are classified as group II. In addition to periosteal reaction and metaphysistis in the long bones, the presence of clavicular fracture makes it important to look for these fractures carefully in other bones without dystrophic changes. Clavicular fracture has been commonly reported occurring as a result of birth trauma, osteogenesis imperfecta and other bone diseases associated with increased bone fragility10 however those in neonates with CS has very limited reporting.
CDC and ACOG recommends universal first trimester screening for syphilis and additional third trimester screening for pregnant women with high risk behavior for syphilis.11 Diagnosis and management of syphilis during pregnancy and in neonatal period have been clearly defined by CDC. Non-uniformity in this practice as seen in the index case including late diagnosis during pregnancy, non-availability of titres of VDRL, RPR and also the non-availability of penicillin has been an issue in certain resource-limited settings. The use of a skeletal survey and early diagnosis of metaphysistis and fracture, along with the qualitative tests as in our case might aid in accurate early diagnosis of CS and initiation of treatment. This might also lead to an earlier resolution of the skeletal changes as seen in this case.
In neonates with congenital syphilis, serology (treponemal and non-treponemal) needs to be repeated at 1, 2, 4, 6 and 12 months.11 At 6 months if non treponemal specific test (NTST) is non reactive and infant remains asymptomatic, no further evaluation or treatment is required. The non treponemal titre is expected to be negative by 12 months after treatment in appropriately treated cases.11 Children with positive titres on follow up are to be considered for the second course of treatment. Long term outcomes in symptomatic CS include increased risk of growth restriction, developmental delay and microcephaly.12 | | | | Conclusion | | Despite universal screening during pregnancy and treatment of latent syphilis in the antenatal period, congenital syphilis can present as only radiological manifestations of metaphysistis which re emphasizes the need for a detailed skeletal survey. Other bone fractures including clavicular fracture need to be carefully identified and treated early for better outcome and reduced morbidity. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Tao, YT., Gao, TY., Li, HY. et al. Global, regional, and national trends of syphilis from 1990 to 2019: the 2019 global burden of disease study. BMC Public Health 23, 754 (2023). https://doi.org/10.1186/s12889-023-15510-4. [CrossRef]
- Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2017. Atlanta, GA: US Department of Health and Human Services; 2018.
- American Academy of Pediatrics. Syphilis. In: Kimberlin DW, Brady MT, Jackson MA, Long SS, editors. Red Book: 2018 Report of the Committee on Infectious Diseases. Grove Village, IL: American Academy of Pediatrics; 2018. p. 773-88.
- Dobson SR. Congenital syphilis: clinical features and diagnosis. In: Kaplan SL, Weisman LE section eds. UpToDate. 2021. Congenital syphilis: clinical features and diagnosis - UpToDate . Accessed 1 Nov 2021.
- Cooper JM, Sánchez PJ. Congenital syphilis. Semin Perinatol. 2018;42(3): 176-184. [CrossRef]
- Singhal P, Patel P, Marfatia YS. A case of congenital syphilis with Hutchinson's triad. Indian J Sex Transm Dis AIDS. 2011 Jan;32(1):34-6. doi: 10.4103/0253-7184.81252. PMID: 21799574; PMCID: PMC3139286. [CrossRef]
- Dai Y, Zhai G, Zhang S, Chen C, Li Z, Shi W. The Clinical Characteristics and Serological Outcomes of Infants With Confirmed or Suspected Congenital Syphilis in Shanghai, China: A Hospital-Based Study. Front Pediatr. 2022 Feb 23;10:802071. doi: 10.3389/fped.2022.802071. PMID: 35281239; PMCID: PMC8904424. [CrossRef]
- Cremin BJ, Fisher RM. The lesions of congenital syphilis. Br J Radiol. 1970;43(509):333-41. [CrossRef]
- Pg Mohammad Hussein PMN, Kew ST, Nang KM, et al. Skeletal manifestations of congenital syphilis: Rare but clinically relevant. Radiol Case Rep. 2021 Oct 1;16(12):3635-3637. doi: 10.1016/j.radcr.2021.09.004. PMID: 34630789; PMCID: PMC8495030. [CrossRef]
- Jenny C, Committee on Child Abuse and Neglect. Evaluating infants and young children with multiple fractures. Pediatrics. 2006;118(3):1299-303. [CrossRef]
- Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR):1-137.
- Lago EG, Vaccari A, Fiori RM. Clinical features and follow-up of congenital syphilis. Sex Transm Dis. 2013;40(2): 85-94. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2026.61
|
| Cite this article as: | | Patel T, Nair S, RR P, Haribalakrishna A. Unusual early skeletal manifestations in a neonate with congenital syphilis. Pediatr Oncall J. 2026;23. doi: 10.7199/ped.oncall.2026.61 |
|