Carolina Fraga1, Inês Aires Martins2, Telma Barbosa3, Célia Azevedo Soares4,5,6,7, Anabela Bandeira8.
1Pediatrics Department, Centro Materno-Infantil do Norte, Centro Hospitalar Universitário de Santo António (CMIN-CHUdSA), Porto, Portugal,
2Pediatrics Department, CMIN-CHUdSA, Porto, Portugal,
3Pediatric Pneumology Department, CMIN-CHUdSA, Porto, Portugal,
4Serviço de Genética Médica, Centro de Genética Médica Jacinto Magalhães, CHUdSA, Porto, Portugal,
5Unit for Multidisciplinary Research in Biomedicine, Instituto de Ciências Biomédicas Abel Salazar/Universidade do Porto, Porto, Portugal,
6Departamento de Ciências Médicas, Universidade de Aveiro, Aveiro, Portugal,
7Institute for Investigation and Innovation in Health (i3S), University of Porto, Porto, Portugal,
8Reference Center for Inherited Disorders of Metabolism, CMIN-CHUdSA, Porto, Portugal.
ADDRESS FOR CORRESPONDENCE
Carolina Fraga, Largo Prof. Abel Salazar 45, 4099-001 Porto, Portugal.
Email: carolinamoraesfraga@gmail.com | | Abstract | Although fractures are common in children, vertebral fractures are exceptional and should raise the suspicion for the presence of osteoporosis. This can be primary, particularly in the presence of positive family history or secondary to chronic illnesses, endocrine disorders or to some drugs.
We report on a 10-year-old boy with asthma controlled with prolonged inhaled corticosteroids who presented with spontaneous vertebral fractures and decreased bone density. There was positive family history for early-onset osteoporosis. A deleterious variant in gene COL1A2 was identified, diagnosing osteogenesis imperfecta. Bone mineral density improved with intravenous bisphosphonates with no further fractures during follow-up period.
Presentation with vertebral fractures is uncommon in COL1A2 osteogenesis imperfecta. Since there are therapeutic options available that might enhance quality of life, further investigation for primary and secondary causes is imperative in the case of osteoporosis in children. | | | | Keywords | | Osteoporosis, Spinal fracture, Adolescent, Pathological fracture. | | | | Introduction | Vertebral fractures in pediatric age are extremely rare, particularly in an otherwise healthy child. Estimated incidence for traumatic vertebral fractures in pediatric age is of 66:1,000,000, though true global incidence is unknown.1 Genetic forms of bone fragility, such as osteogenesis imperfecta (OI), can play a role in increasing the susceptibility to vertebral fractures. OI is a connective tissue disorder primarily, with an incidence between 1:13,500 and 1:9,700, caused by deleterious variants in either COL1A1 or COL1A2 genes. Another form of OI, resulting from deleterious variants in the PLS3 gene, is characterized by a predominance of vertebral fractures and follows an X-linked inheritance pattern.2,3
OI exhibits a wide range of phenotypic variations, including mild to severe and even lethal forms, often involving multiple systems. It is associated with significant morbidity, negatively affected life quality and decreased life expectancy.3
| | | | Case Report | A 10-year-old boy was referred to Inherited Metabolic Diseases Consultation due to severe spine osteoporosis. He had allergic asthma, diagnosed when he was 6 years-old, controlled with inhaled low dose corticosteroid during the fall and winter months. He practiced swimming and karate without history of fractures. Family history indicated a pattern of early onset osteoporosis: the mother was diagnosed at 36 years-old and the maternal grandmother at 40 years.
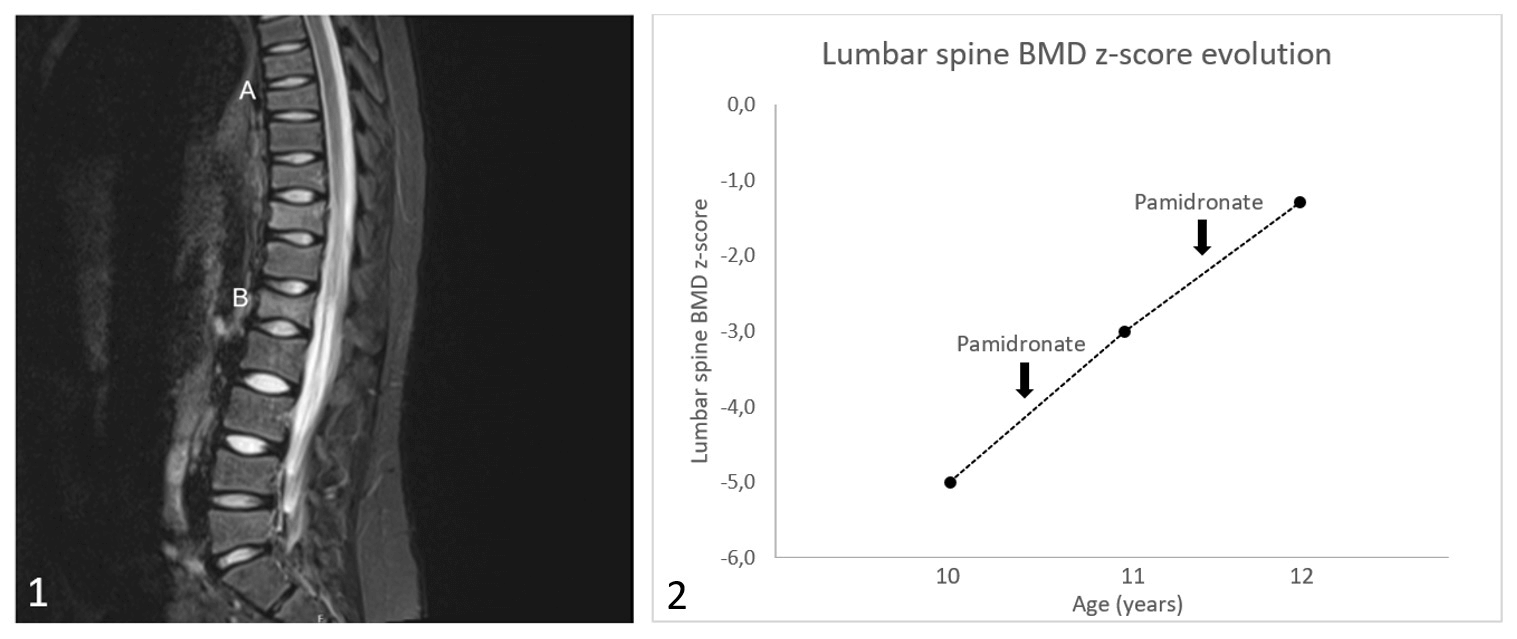
Following a weight gain as a result of sedentary lifestyle, he reported experiencing low back pain without any known trauma. X-ray revealed the presence of two vertebral fractures at the T11 and L1 levels, along with a significant decrease in bone density. Magnetic resonance imaging (MRI) confirmed the presence of the two recent fractures, showing a 40% loss of vertebral height ratio (Figure 1) and, additionally, revealed vertebral wedging in T6-T9, indicating the likely occurrence of previous fractures.
Figure 1. 1 - Spinal Magnetic Resonance: A. Wedging of vertebral bodies T6, T7, T8 e T9 in relation to chronic fractures. B. Shorting of vertebral height of L1 body in approximately 40%, in relation to recent fracture. 2 – Graph of Bone mineral density z-score evolution with pamidronate administration timings.
He denied other symptoms and the consumption of other drugs. On physical examination, discrete blue sclera was noted, dentition and muscle strength were normal and no other skeletal deformities were apparent. Height was in the 75th percentile and body mass index was 21 Kg/m2 (95th percentile).
Bone density scan confirmed very low bone mineral density (0.304 g/cm2), with Z-score of -5.0 for lumbar density (Figure 1). Secondary causes of osteoporosis were excluded through lab results. Skeletal X-ray did not document other fractures. He was started on vitamin D and calcium oral supplementation and contact sports were advised against.
Due to the notable predominance of spine fractures and the observed inheritance pattern from the matrilineal lineage, a high suspicion was raised for a genetic form of bone fragility. In order to investigate genes linked to bone fragility, a skeletal dysplasia gene panel analysis was conducted. Subsequently, a heterozygous variant, c.757G>T p. (Gly253Cys), in the COL1A2 gene was identified. After co-segregation with the phenotype within the family, this variant was classified as likely pathogenic.
After two cycles of intravenous pamidronate, with six months interval, the bone density Scan improved to a density (0.566 g/cm2), with Z-score -1.3 for lumbar density (Figure 1). No other fractures were reported in the following two years of follow-up.
| | | | Discussion | While fractures are very frequent in childhood, vertebral fractures are uncommon in an otherwise healthy child.1 The reported child had no previous history of fractures or of major trauma, but presented multiple vertebral fractures with evidence of osteopenia. In such cases, both primary and secondary causes should be considered. The approach of osteoporosis includes a routine measurement of bone metabolism and the assessment of bone mass by dual energy X-ray absorptiometry (DEXA). Secondary causes are evaluated by clinical history, physical examination and laboratory investigations. Genetic studies should be considered in the presence of clinically significant fracture history and in the absence of a secondary cause.5 This child was active, without symptoms of chronic inflammatory disease or consumption of potentially osteotoxic drugs, apart from low-dose inhaled corticosteroids (ICS) which, unlike high dose long-term ICS, have no influence on BMD.6 The family history of middle-aged onset of osteoporosis raised the suspicion of a primary cause.
A likely pathogenic variant in heterozygosity in the COL1A2 gene was identified which segregated in the mother and grandmother, both having documented osteoporosis of undetermined etiology. COL1A2 may present as different clinical types and with variable severity.3
Management of osteoporosis aims to improve function, mobility and pain and prevent further fractures, requiring a multidisciplinary approach. High impact physical activities and contact sports should be avoided. Oral supplementation with vitamin D and calcium may be necessary.5 Pharmacological treatment in OI is based on bisphosphonates (BP) which improve BMD, reduce fracture incidence and in children, may have a role in reshaping of fractured vertebrae. Intravenous BP are better tolerated than oral, intravenous pamidronate being the most widely used in children. In the reported case, treatment with BP resulted in 85.9% improvement of BMD and no fractures. Genetic counselling should be offered to affected families.
In conclusion, the presence of a vertebral fracture in a child always requires further investigation. Bisphosphonates in OI increase BMD and reduce the incidence of fractures and therefore a timely diagnosis is crucial to start the proper treatment.
List of abbreviations
- BMD - bone mineral density
- BP – bisphosphonates
- DEXA – dual energy X-ray absorptiometry
- ICS – inhaled corticosteroids
- OI - Osteogenesis imperfecta
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Clark EM. The epidemiology of fractures in otherwise healthy children. Curr Osteoporos Rep. 2014 Sep;12(3):272-8. doi: 10.1007/s11914-014-0227-y. [CrossRef]
- Yang L, Liu B, Dong X, Wu J, Sun C, Xi L, et al. Clinical severity prediction in children with osteogenesis imperfecta caused by COL1A1/2 defects. Osteoporos Int. 2022 Jun;33(6):1373-1384. doi: 10.1007/s00198-021-06263-0. Epub 2022 Jan 19. [CrossRef]
- Tauer JT, Robinson ME, Rauch F. Osteogenesis Imperfecta: New Perspectives From Clinical and Translational Research. JBMR Plus. 2019 Feb 20;3(8):e10174. doi: 10.1002/jbm4.10174. [CrossRef]
- Saraff V, Högler W. ENDOCRINOLOGY AND ADOLESCENCE: Osteoporosis in children: diagnosis and management. Eur J Endocrinol. 2015 Dec;173(6):R185-97. doi: 10.1530/EJE-14-0865. [CrossRef]
- Ciancia S, van Rijn RR, Högler W, Appelman-Dijkstra NM, Boot AM, Sas TCJ, et al. Osteoporosis in children and adolescents: when to suspect and how to diagnose it. Eur J Pediatr. 2022 Jul;181(7):2549-2561. doi: 10.1007/s00431-022-04455-2. Epub 2022 Apr 6. [CrossRef]
- Kwda A, Gldc P, Baui B, Kasr K, Us H, S W, et al. Effect of long term inhaled corticosteroid therapy on adrenal suppression, growth and bone health in children with asthma. BMC Pediatr. 2019 Nov 5;19(1):411. doi: 10.1186/s12887-019-1760-8. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2026.4
|
| Cite this article as: | | Fraga C, Martins I A, Barbosa T, Soares C A, Bandeira A. Atypical predominance of vertebral fractures as the first sign of COL1A2-related osteogenesis imperfecta. Pediatr Oncall J. 2026;23: 34-35. doi: 10.7199/ped.oncall.2026.4 |
|