Leonor Cardoso1, Patrícia Dias Santos2, Rosário Stilwell2, Claúdia Rodrigues3, Ema Santos4, Joana Patena Forte4, Pedro Morais4, Maria Costa5, Madalena Borges5, Rute Baeta Baptista5,6, Telma Francisco5,6, Gisela Neto5, Sofia Lima4, Aline Vaz Silva4, Vanda Pratas Vital4, Dinorah Cardoso4, Fátima Alves4, Margarida Abranches5.
1Department of Paediatrics, Unidade Local de Saúde da Cova da Beira, Covilhã, Portugal,
2Department of Paediatrics, Hospital Dona Estefânia, Unidade Local de Saúde São José, Centro Clínico Académico de Lisboa, Lisboa, Portugal,
3Department of Paediatrics, Unidade Local de Saúde Médio Tejo, Torres Novas, Portugal,
4Paediatric Urology Unit, Hospital Dona Estefânia, Unidade Local de Saúde São José, Centro Clínico Académico de Lisboa, Lisboa, Portugal,
5Paediatric Nephrology Unit, Hospital Dona Estefânia, Unidade Local de Saúde São José, Centro Clínico Académico de Lisboa, Lisboa, Portugal,
6NOVA Medical School, Faculdade de Ciências Médicas, NMS, FCM, Universidade Nova de Lisboa, Centro Clínico Académico de Lisboa, Lisboa, Portugal.
ADDRESS FOR CORRESPONDENCE
Rute Baeta Baptista, Hospital Dona Estefânia, Rua Jacinta Marto, 1169-045 Lisbon, Portugal.
Email: rute.baeta.baptista@gmail.com | | Abstract | Background: Posterior urethral valves (PUV) affect 1 in 5,000 live male births, with 8–21% progressing to end-stage kidney disease (ESKD) within ten years. Early predictors of adverse kidney outcomes in PUV are poorly defined.
Methods: A retrospective cohort study was conducted on children who underwent PUV ablation at a single center from January 2015 to June 2022. Patients with less than six months of follow-up were excluded. The primary outcome was a composite of low estimated glomerular filtration rate (eGFR) for age or the need for kidney replacement therapy (KRT).
Results: Among 41 patients, 24 (59%) were diagnosed prenatally and 14 (34%) were referred from other countries. Prenatally diagnosed patients were more likely to be born preterm (50% vs. 12%, p = 0.006) and had higher baseline serum creatinine (0.66 [IQR 0.49-2.45] vs. 0.52 [IQR 0.44-0.54] mg/dL; p = 0.036). Over a median follow-up of 3.1 years, 13 patients (32%) met the primary outcome, including three requiring peritoneal dialysis, all born preterm. Logistic regression analyses, adjusted for age at last follow-up, identified prenatal diagnosis (OR 7.49; 95% CI 1.18-47.56; p = 0.033), prematurity (OR 18.59; 95% CI 2.63-131.50; p = 0.003 and high pre-ablation serum creatinine (OR 5.88; 95% CI 1.19-28.97; p = 0.029) as significant predictors of adverse outcomes.
Conclusion: Nearly one-third of the cohort experienced a decline in eGFR or required KRT. Prenatal diagnosis, prematurity and elevated pre-ablation serum creatinine were significant predictors of adverse kidney outcomes in children with PUV.
| | | | Keywords | Chronic kidney disease, Kidney outcomes, Posterior urethral valves, Prognosis, Children, Adolescent.
Abbreviations:
CKD – Chronic kidney disease
CI – Confidence interval
ESKD – End-stage kidney disease
eGFR – Estimated glomerular filtration rate
IQR – Interquartile range
KRT – Kidney replacement therapy
OR – Odds ratio
PALOP – Portuguese-speaking African countries
PUV – Posterior urethral valves
SD – Standard deviations
ULN – Upper limit of normal
UTD – Urinary tract dilatation
UTI – Urinary tract infection
VUR – Vesicoureteral reflux
| | | | Introduction | Posterior urethral valves (PUV) are a congenital anomaly of the urinary tract found exclusively in male patients, with an incidence of approximately 1 in 5,000 live male births.1,2 These membranous folds within the posterior urethra obstruct urine flow, potentially leading to severe complications. Although the precise embryological mechanism underlying PUV remains unclear, it likely involves disruptions in the development of the male urethra during fetal growth.3
As the most severe form of pediatric obstructive uropathy, PUV is a leading cause of chronic kidney disease (CKD) in children. Up to 65% of affected individuals develop CKD, with 8–21% progressing to end-stage kidney disease (ESKD) by the age of ten.4,5 This underscores the importance of identifying early predictive factors for adverse kidney outcomes.
CKD in PUV is driven by a combination of congenital kidney dysplasia and acquired kidney injury, often resulting from poor bladder function and infections. Bladder dysfunction contributes to urinary stasis and progressive renal parenchymal damage.6 Prenatal ultrasound findings, such as severe bilateral hydronephrosis, oligohydramnios or features suggestive of kidney dysplasia, particularly when identified before 24 weeks of gestation, are associated with an increased risk of perinatal mortality and CKD.7,8
This study aims to investigate predictors of kidney outcomes in children with PUV, focusing on markers that can inform risk stratification and guide clinical management. By understanding these factors more comprehensively, we aim to improve kidney outcomes in children with PUV through targeted interventions and personalized care strategies. | | | | Methods | Study design and population
This retrospective, single-center cohort study was conducted at a level III care university hospital. All patients aged 0-18 years diagnosed with posterior urethral valves (PUV) who underwent ablation at our center between January 1, 2015 and June 30, 2022 were eligible for inclusion. Patients with less than six months of follow-up were excluded.
Data analyzed
Data were collected through a review of electronic medical records. Key patient information included country of birth, gestational age, birth weight, need for neonatal resuscitation and comorbidities. The timing of diagnosis (prenatal or postnatal), findings leading to a prenatal diagnosis and clinical presentation of postnatally diagnosed cases were documented. Initial postnatal ultrasound findings and results from preoperative cystography (e.g., vesicoureteral reflux and post-void residual volume) were analyzed.
Management data included the age at first urethral catheterization, age at endoscopic PUV ablation and any interventions performed before or at the time of PUV ablation (e.g., vesicostomy or high diversion). Post-ablation interventions, such as endoscopic re-ablation of residual PUV, were also recorded.
Perioperative PUV ablation metrics included maximum serum creatinine levels before surgery, nadir creatinine levels within the first week after ablation and pre- and postoperative estimated glomerular filtration rate (eGFR).
The primary outcome was a composite of low eGFR for age or the need for kidney replacement therapy (KRT). Low eGFR for age was defined as eGFR <90 mL/min/1.73m2, for children older than two years and eGFR below two standard deviations (SD) below the mean for children under two years, calculated using the bedside serum creatinine Schwartz formula.
Other outcomes assessed included the presence of vesicoureteral reflux (VUR), post-void residual volume and significant renal scarring on dimercaptosuccinic acid (DMSA) renal scintigraphy.
Statistical methods
Continuous variables were summarized using means and standard deviations (SD) or medians and interquartile ranges (IQR), depending on the distribution of the data. Categorical variables were reported as frequencies and percentages.
Comparisons between groups were made using independent t-tests for normally distributed continuous variables and Mann-Whitney U tests for non-normally distributed continuous variables. For categorical variables, Chi-square tests or Fisher’s exact tests were applied as appropriate.
Univariate logistic regression analyses were conducted to identify predictors of adverse kidney outcomes. These analyses were subsequently adjusted for age at the last follow-up visit. A multivariate logistic regression model, including all significant predictors identified in univariate analyses and adjusted for age at the last follow-up, was also performed. Odds ratios (OR) and 95% confidence intervals (CI) were calculated for all regression models. A two-tailed p-value of <0.05 was considered statistically significant.
All statistical analyses were performed using Stata® version 14.0 (StataCorp).
Ethical considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki. As a retrospective observational study using anonymized data collected as part of routine clinical care, it was exempt from formal ethical approval. Informed consent was not required due to the retrospective nature of the data collection and the anonymization of patient information. All data were handled and analyzed in compliance with data protection regulations to safeguard confidentiality and privacy. | | | | Results | We identified 45 patients who underwent PUV ablation at the study institution between January 1, 2015 and June 30, 2022. After excluding four patients with a follow-up period of less than six months, the final cohort consisted of 41 patients. Most patients were diagnosed prenatally (54%) and the majority (66%) were from Portugal. Fourteen patients (34%) were born prematurely and four (10%) required neonatal resuscitation. In addition to prematurity, relevant comorbidities were identified in 10 patients (24%), including sickle cell disease (6), trisomy 21 (2), nephroblastoma (1) and ureterocele with ureteral duplication (1). Regarding the timing of diagnosis, the median gestational age at the first abnormal prenatal scan for patients with a prenatal diagnosis of PUV was 29 (IQR 22–34) weeks, with a range from 12 to 36 weeks. For patients diagnosed postnatally, the median age at diagnosis ranged from 0 days to 9 years, with a median of 3.84 months (IQR 11.00 days to 4.71 years). Overall, the median peak serum creatinine before ablation was 0.54 (IQR 0.46–1.03; range 0.37–6.27) mg/dL (Table 1).
Table 1. Demographic and clinical characteristics of the study population.
| Characteristics |
N = 41 |
| Timing of diagnosis, n (%) |
|
| Prenatal diagnosis |
24 (59) |
| Postnatal diagnosis |
17 (41) |
| Country of origin, n (%) |
|
| Portugal |
27 (66) |
| PALOP |
12 (29) |
| Brazil |
2 (5) |
| Birth gestational age (weeks), median (IQR) |
38 (36–39) |
| Birth weight (grams), median (IQR) |
3007 (2515–3480) |
| Need for neonatal resuscitation, n (%) |
4 (10) |
| Prematurity, n (%) |
14 (34) |
| Comorbidities excluding prematurity, n (%) |
10 (24) |
| Peak serum creatinine before PUV ablation (mg/dL), median (IQR) |
0.54 (0.46-1.03) |
| Gestational age at first abnormal prenatal scan in patients with prenatal diagnosis of PUV (weeks), median (IQR) |
28.5 (21.5-33.5) |
| Age at diagnosis in patients diagnosed postnatally (months), median (IQR) |
3.80 (0.36-56.52) |
IQR – interquartile range; PALOP – Portuguese-speaking African countries.
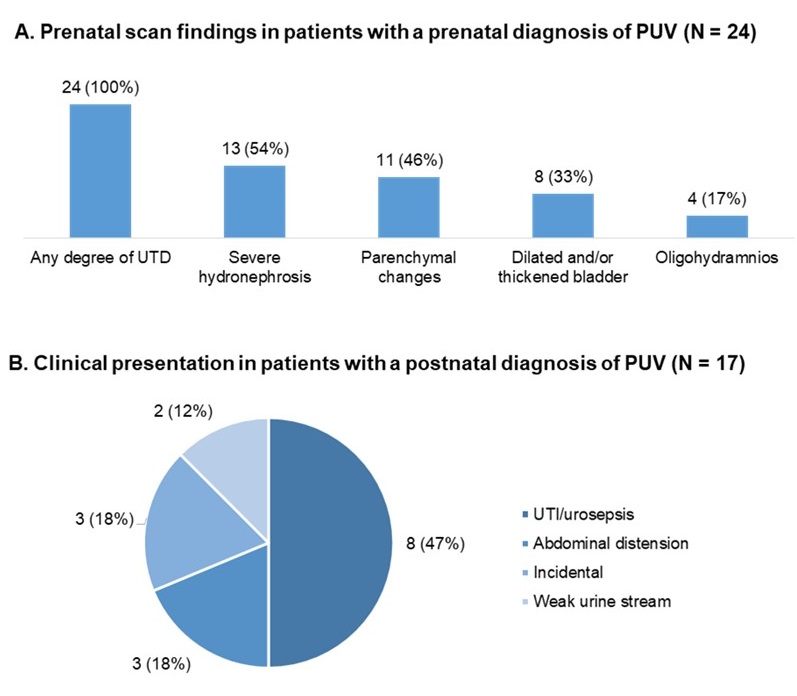
Clinical presentation based on the timing of diagnosis is illustrated in Figure 1. Among the 24 (59%) children diagnosed prenatally, 13 (54%) presented with severe hydronephrosis, 11 (46%) showed kidney parenchymal changes and 4 (17%) were diagnosed with oligohydramnios on prenatal ultrasound scans. The majority of the 17 (41%) children diagnosed postnatally were symptomatic. The most common indications for imaging were urinary tract infection or urosepsis (8, 47%), followed by abdominal distention (3, 18%) and weak urine stream (2, 12%). Notably, three children (18%) had PUV discovered incidentally during an ultrasound performed for other reasons.
Figure 1. Clinical presentation by the timing of diagnosis.
A. Prenatal scan findings in patients with a prenatal diagnosis of PUV.
B. Clinical presentation in patients with a postnatal diagnosis of PUV.
PUV – posterior urethral valves; UTD – urinary tract dilatation; UTI – urinary tract infection.
A comparison of clinical patient characteristics and interventions based on the timing of PUV diagnosis is shown in Table 2. Patients with a prenatal diagnosis were more frequently born preterm (12 [50%] versus 2 [12%]; p = 0.006), had higher peak serum creatinine before PUV ablation (0.66 [IQR 0.49–2.45] versus 0.52 [IQR 0.44–0.54] mg/dL; p = 0.036) and were more likely to have a dilated posterior urethra on postnatal ultrasound scans (12 [50%] versus 3 [18%]; p = 0.041).
Table 2. Clinical patient characteristics and interventions by timing of PUV diagnosis: prenatal versus postnatal.
| |
All (N = 41) |
Prenatal diagnosis
(N = 24) |
Postnatal diagnosis
(N = 17) |
P value |
| PRIMARY OUTCOME* |
13 (32) |
10 (42) |
3 (18) |
0.024 |
| SECONDARY OUTCOMES |
|
| eGFR below expected for age, n (%)* |
10 (24) |
8 (33) |
3 (18) |
0.014 |
| Kidney replacement therapy, n (%) |
3 (7) |
2 (8) |
0 |
0.210 |
| eGFR at last follow-up visit (mL/min/1.73 m2), median (IQR)* |
95.4 (79.2-115.1) |
80.0 (36.0-97.0) |
101.0 (90.0-126.0) |
0.014 |
| Nadir serum creatinine (mg/dL), median (IQR) |
0.48 (0.42-0.73) |
0.57 (0.40-1.18) |
0.46 (0.42-0.57) |
0.340 |
| Nadir serum creatinine >1 mg/dL, n (%) |
6 (15) |
5 (21) |
1 (6) |
0.150 |
| VUR in the first post ablation cystography, n (%) |
15 (37) |
7 (29) |
8 (47) |
0.160 |
| Bilateral VUR |
7 (17) |
6 (25) |
1 (6) |
0.060 |
| Post voiding residue |
2 (5) |
2 (8) |
0 (0) |
0.140 |
| Any degree of renal scarring in the last available scintigraphy, n (%) |
11 (27) |
6 (25) |
5 (29) |
0.300 |
| Bilateral renal scarring |
9 (22) |
5 (21) |
4 (24) |
0.500 |
| Relative renal function =40% |
10 (24) |
6 (25) |
4 (24) |
0.120 |
*excluding patients on KRT for the eGFR calculation.
eGFR – estimated glomerular filtration rate; IQR – interquartile range; KRT – kidney replacement therapy; PUV – posterior urethral valves; VUR – vesicoureteral reflux.
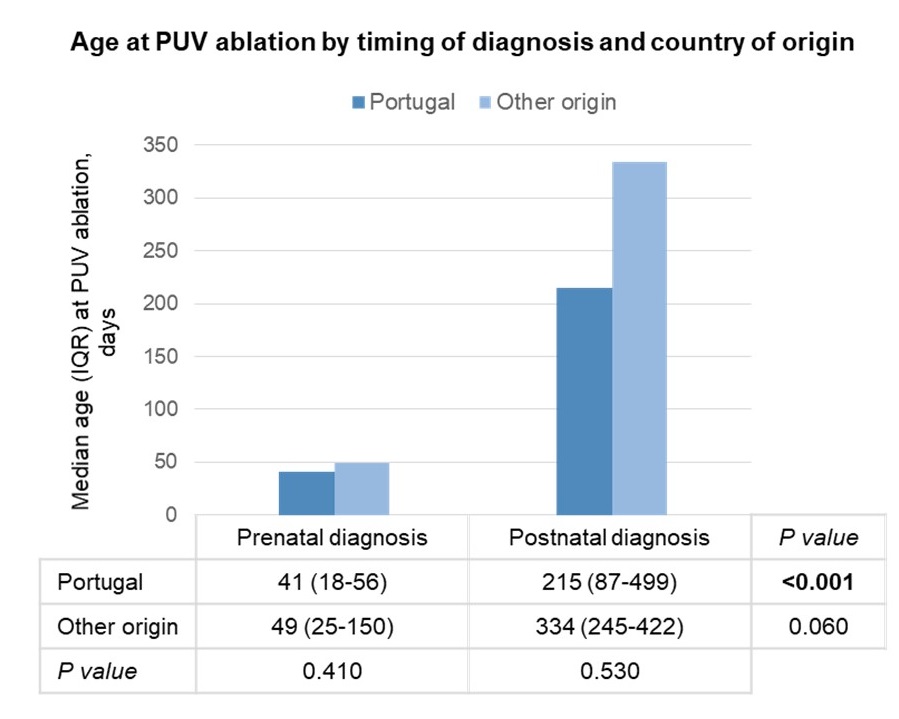
Notably, during the study period, the median age at PUV ablation varied widely based on the timing of diagnosis and country of origin (Figure 2). Overall, patients with a prenatal diagnosis underwent PUV ablation at a younger age than those with a postnatal diagnosis (45 [IQR 24–62] days versus 9 [IQR 3.25–16.07] months; p < 0.001). Additionally, patients born in Portugal tended to undergo ablation at a younger age than those referred from other countries. Initial management included immediate bladder drainage for all patients via a feeding tube or Foley catheter upon suspicion or confirmation of PUV. As expected, patients diagnosed prenatally underwent their first urethral catheter placement at a significantly younger age than those diagnosed postnatally (0 [IQR 0–5] versus 82 [IQR 15–123] days; p <0.001). Prior to April 2021, when the hospital acquired a neonatal resectoscope, patients were gradually catheterized with progressively larger catheters until they could tolerate a 9 Fr catheter, after which they proceeded to PUV ablation with the smallest available resectoscope at the time. Since April 2021, the median age at primary PUV ablation for the three term-born patients with a prenatal diagnosis from Portugal has been reduced to 7 days.
Figure 2. Age (in days) at PUV ablation by timing of diagnosis and country of origin.
IQR – interquartile range; PUV – posterior urethral valves.
Note: Since the acquisition of a neonatal resectoscope in April 2021, the median age at primary PUV ablation for the three patients with a prenatal diagnosis born at term in Portugal was 7 days.
The median follow-up duration was 3.08 years (IQR: 24.96 months to 3.99 years) and the median age at the latest follow-up was 3.1 (IQR: 2.1–4.0) years. The primary outcome was met by 13 (32%) patients in the overall cohort, with a significantly higher rate among those with a prenatal diagnosis compared to those diagnosed postnatally (10 [42%] vs. 3 [18%]; p = 0.024). Three children (7%) required peritoneal dialysis and an additional ten (24%) had an eGFR lower than expected for their age. Notably, 10 (45%) of prenatally diagnosed children achieved the composite renal outcome, whereas only 3 (17%) of postnatally diagnosed children met the primary outcome. Among the three patients who underwent KRT, two were diagnosed prenatally and all three were born prematurely. The maximum serum creatinine values recorded prior to PUV ablation were 1.15 mg/dL, 4.24 mg/dL and 6.27 mg/dL, while the nadir serum creatinine values were 0.86 mg/dL, 4.08 mg/dL and 5.59 mg/dL, respectively. The mean eGFR at the end of follow-up, excluding patients on KRT, was 95 (IQR: 79–115) mL/min/1.73 m2, which was significantly lower for patients with a prenatal diagnosis than for those diagnosed postnatally (80 [IQR: 36–97] vs. 101 [IQR: 90–126] mL/min/1.73 m2; p = 0.014). Other secondary outcomes included post-ablation vesicoureteral reflux in 15 (37%) patients, any degree of renal scarring in 11 (27%) children and relative renal function of 40% or less in 10 (24%) patients (Table 3).
Table 3. Patient outcomes in the overall cohort and stratified by timing of PUV diagnosis (prenatal versus postnatal).
| |
All (N = 41) |
Prenatal diagnosis
(N = 24) |
Postnatal diagnosis
(N = 17) |
P value |
| PRIMARY OUTCOME* |
13 (32) |
10 (42) |
3 (18) |
0.024 |
| SECONDARY OUTCOMES |
|
| eGFR below expected for age, n (%)* |
10 (24) |
8 (33) |
3 (18) |
0.014 |
| Kidney replacement therapy, n (%) |
3 (7) |
2 (8) |
0 |
0.210 |
| eGFR at last follow-up visit (mL/min/1.73 m2), median (IQR)* |
95.4 (79.2-115.1) |
80.0 (36.0-97.0) |
101.0 (90.0-126.0) |
0.014 |
| Nadir serum creatinine (mg/dL), median (IQR) |
0.48 (0.42-0.73) |
0.57 (0.40-1.18) |
0.46 (0.42-0.57) |
0.340 |
| Nadir serum creatinine >1 mg/dL, n (%) |
6 (15) |
5 (21) |
1 (6) |
0.150 |
| VUR in the first post ablation cystography, n (%) |
15 (37) |
7 (29) |
8 (47) |
0.160 |
| Bilateral VUR |
7 (17) |
6 (25) |
1 (6) |
0.060 |
| Post voiding residue |
2 (5) |
2 (8) |
0 (0) |
0.140 |
| Any degree of renal scarring in the last available scintigraphy, n (%) |
11 (27) |
6 (25) |
5 (29) |
0.300 |
| Bilateral renal scarring |
9 (22) |
5 (21) |
4 (24) |
0.500 |
| Relative renal function =40% |
10 (24) |
6 (25) |
4 (24) |
0.120 |
*excluding patients on KRT for the eGFR calculation.
eGFR – estimated glomerular filtration rate; IQR – interquartile range; KRT – kidney replacement therapy; PUV – posterior urethral valves; VUR – vesicoureteral reflux.
Prenatal diagnosis, prematurity and pre-ablation serum creatinine values above the upper limit of normal were identified as predictors of low eGFR for age or the need for KRT in univariate logistic regression analyses. These predictors remained significant after adjusting for age at the last follow-up. However, none of these predictors remained significant in the multivariate model adjusted for age at the last follow-up, which included all three predictors (Table 4).
Table 4. Predictors of low eGFR for age or need for kidney replacement therapy in the overall cohort of children with PUV.
| |
OR/coefficient |
95% CI |
P value |
| Unadjusted univariate regression |
|
| Prenatal diagnosis |
6.25 |
1.14-34.12 |
0.034 |
| Prematurity |
8.63 |
1.96-37.94 |
0.004 |
| Pre-ablation serum creatinine levels above the ULN |
7.70 |
1.40-42.44 |
0.019 |
| Age-adjusted univariate regression |
|
| Prenatal diagnosis |
7.49 |
1.18-47.56 |
0.033 |
| Prematurity |
18.59 |
2.63-131.50 |
0.003 |
| Pre-ablation serum creatinine levels above the ULN |
5.88 |
1.19-28.97 |
0.029 |
| Age-adjusted multivariate regression model |
|
| Prenatal diagnosis |
1.29 |
0.11-15.6 |
0.842 |
| Prematurity |
3.60 |
0.26-49.1 |
0.337 |
| Pre-ablation serum creatinine levels above the ULN |
3.46 |
0.66-18.1 |
0.142 |
CI – confidence interval; OR – odds ratio; PUV – posterior urethral valves; ULN – upper limit of normal
| | | | Discussion | This study aimed to assess kidney outcomes in children with PUV treated at a single institution over 7.5 years and identify predictors of poor kidney outcomes. Nearly one-third of our cohort experienced a decline in eGFR below the expected range for age or required KRT over a median follow-up of 3 years. We identified prenatal diagnosis, prematurity and pre-ablation serum creatinine levels above the upper limit of normal as significant predictors of worse kidney outcomes. These findings are consistent with those from other published cohorts.9,10
Our findings suggest a clustering of risk factors among children with worse kidney outcomes, as patients diagnosed prenatally were more likely to be born prematurely and had higher peak serum creatinine levels prior to PUV ablation compared to those diagnosed postnatally. This clustering of risk factors may have contributed to the lack of improvement in outcomes despite earlier diagnosis and intervention. As expected, prenatal diagnosis was frequently associated with severe hydronephrosis, kidney parenchymal changes and oligohydramnios, all factors that have been identified as prenatal markers of worse long-term kidney outcomes in studies with longer follow-up.5,11 This suggests that PUV is often detected earlier (in utero) in more severe cases. In contrast, postnatally diagnosed patients are more likely to have partial obstruction and a milder course, as evidenced by the three postnatal cases diagnosed incidentally in our cohort. One of the most significant changes in clinical practice during the study period was the acquisition of a neonatal resectoscope in April 2021, which enabled earlier PUV ablation. This advancement may improve outcomes for some children by reducing the duration of obstruction and allowing for earlier intervention. However, the overall impact on outcomes remains uncertain and continued follow-up is essential to assess the long-term benefits of early intervention. The higher incidence of adverse kidney outcomes in the prenatal diagnosis group, despite earlier first urine drainage and PUV ablation, highlights that earlier desobstruction does not necessarily guarantee optimal outcomes.12,13,14
Among the three patients requiring peritoneal dialysis, two were diagnosed prenatally, all were born prematurely and all had significantly elevated pre-ablation serum creatinine levels. Additionally, the nadir creatinine in the first week following PUV ablation was higher than 0.70 mg/dL for all of them, which aligns with the consistent finding in the literature that nadir creatinine is the best prognostic factor for long-term renal function in patients affected by PUV.5,15,16 Unfortunately, we were unable to consistently capture nadir creatinine during the first year due to shared care with local hospitals and had to limit our analysis to nadir creatinine in the first week following PUV ablation, which was consistently documented for all patients in the cohort.
While this study provides valuable insights into the factors influencing renal outcomes in children with PUV, it is limited by its retrospective design, single-center nature, relatively small sample size and short duration of follow-up. Additionally, we were unable to capture detailed data on all potential confounding factors, such as post-ablation pharmacologic management strategies, urinary tract infections, bladder dysfunction, need for clean intermittent catheterization or other long-term complications.
In conclusion, nearly one-third of our cohort experienced a decline in eGFR below the expected range for age or required KRT over a median follow-up period of 3 years. We identified prenatal diagnosis, prematurity and elevated pre-ablation serum creatinine as predictors of worse kidney outcomes in children with PUV. Improving outcomes for higher-risk children remains challenging, as the clustering of these risk factors may limit the potential benefits of early detection and intervention in PUV. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Thakkar D, Deshpande AV, Kennedy SE. Epidemiology and demography of recently diagnosed cases of posterior urethral valves. Pediatr Res. 2014 Dec;76(6):560-3. doi: 10.1038/pr.2014.134. Epub 2014 Sep 8. PMID: 25198372. [CrossRef] [PubMed]
- Brownlee E, Wragg R, Robb A, Chandran H, Knight M, McCarthy L; BAPS-CASS. Current epidemiology and antenatal presentation of posterior urethral valves: Outcome of BAPS CASS National Audit. J Pediatr Surg. 2019 Feb;54(2):318-321. doi: 10.1016/j.jpedsurg.2018.10.091. Epub 2018 Nov 7. PMID: 30528204. [CrossRef] [PubMed]
- Krishnan A, de Souza A, Konijeti R, Baskin LS. The anatomy and embryology of posterior urethral valves. J Urol. 2006 Apr;175(4):1214-20. doi: 10.1016/S0022-5347(05)00642-7. PMID: 16515962. [CrossRef] [PubMed]
- Bain A, Lavoie C, Rodriguez-Lopez S, Kiddoo D. Renal outcomes of children born with posterior urethral valves at a tertiary center: A 15-year retrospective review. Can Urol Assoc J. 2023 Apr;17(4):111-116. doi: 10.5489/cuaj.8102. PMID: 36486177; PMCID: PMC10073527. [CrossRef] [PubMed] [PMC free article]
- Meneghesso D, Bertazza Partigiani N, Spagnol R, Brazzale AR, Morlacco A, Vidal E. Nadir creatinine as a predictor of renal outcomes in PUVs: A systematic review and meta-analysis. Front Pediatr. 2023 Mar 15;11:1085143. doi: 10.3389/fped.2023.1085143. PMID: 37009274; PMCID: PMC10050680. [CrossRef] [PubMed] [PMC free article]
- Hennus PM, van der Heijden GJ, Bosch JL, de Jong TP, de Kort LM. A systematic review on renal and bladder dysfunction after endoscopic treatment of infravesical obstruction in boys. PLoS One. 2012;7(9):e44663. doi: 10.1371/journal.pone.0044663. Epub 2012 Sep 13. PMID: 23028576; PMCID: PMC3441498. [CrossRef] [PubMed] [PMC free article]
- Morris RK, Malin GL, Quinlan-Jones E, Middleton LJ, Hemming K, Burke D, Daniels JP, Khan KS, Deeks J, Kilby MD; Percutaneous vesicoamniotic shunting in Lower Urinary Tract Obstruction (PLUTO) Collaborative Group. Percutaneous vesicoamniotic shunting versus conservative management for fetal lower urinary tract obstruction (PLUTO): a randomised trial. Lancet. 2013 Nov 2;382(9903):1496-506. doi: 10.1016/S0140-6736(13)60992-7. Epub 2013 Aug 14. PMID: 23953766; PMCID: PMC3898962. [CrossRef] [PubMed]
- Capone V, Persico N, Berrettini A, Decramer S, De Marco EA, De Palma D, Familiari A, Feitz W, Herthelius M, Kazlauskas V, Liebau M, Manzoni G, Maternik M, Mosiello G, Schanstra JP, Vande Walle J, Wühl E, Ylinen E, Zurowska A, Schaefer F, Montini G. Definition, diagnosis and management of fetal lower urinary tract obstruction: consensus of the ERKNet CAKUT-Obstructive Uropathy Work Group. Nat Rev Urol. 2022 May;19(5):295-303. doi: 10.1038/s41585-022-00563-8. Epub 2022 Feb 8. PMID: 35136187. [CrossRef] [PubMed]
- Matsell DG, Catapang M, Becknell B. Predicting outcomes in children with congenital anomalies of the kidney and urinary tract. Pediatr Nephrol. 2023 Oct;38(10):3407-3415. doi: 10.1007/s00467-023-05992-0. Epub 2023 May 3. PMID: 37133803; PMCID: PMC10962402. [CrossRef] [PubMed] [PMC free article]
- Bilgutay AN, Roth DR, Gonzales ET Jr, Janzen N, Zhang W, Koh CJ, Gargollo P, Seth A. Posterior urethral valves: Risk factors for progression to renal failure. J Pediatr Urol. 2016 Jun;12(3):179.e1-7. doi: 10.1016/j.jpurol.2015.10.009. Epub 2015 Nov 26. PMID: 26705688; PMCID: PMC4882264. [CrossRef] [PubMed] [PMC free article]
- Herbst KW, Tomlinson P, Lockwood G, Mosha MH, Wang Z, D'Alessandri-Silva C. Survival and Kidney Outcomes of Children with an Early Diagnosis of Posterior Urethral Valves. Clin J Am Soc Nephrol. 2019 Nov 7;14(11):1572-1580. doi: 10.2215/CJN.04350419. Epub 2019 Oct 3. PMID: 31582461; PMCID: PMC6832049. [CrossRef] [PubMed] [PMC free article]
- Sarhan OM, Helmy TE, Alotay AA, Alghanbar MS, Nakshabandi ZM, Hafez AT. Did antenatal diagnosis protect against chronic kidney disease in patients with posterior urethral valves? A multicenter study. Urology. 2013 Dec;82(6):1405-9. doi: 10.1016/j.urology.2013.07.058. Epub 2013 Oct 16. PMID: 24139350. [CrossRef] [PubMed]
- Kibar Y, Ashley RA, Roth CC, Frimberger D, Kropp BP. Timing of posterior urethral valve diagnosis and its impact on clinical outcome. J Pediatr Urol. 2011 Oct;7(5):538-42. doi: 10.1016/j.jpurol.2010.08.002. Epub 2010 Sep 9. PMID: 20829118. [CrossRef] [PubMed]
- Yadav P, Rickard M, Kim JK, Richter J, Lolas M, Alshammari D, Chua ME, Dos Santos J, Lorenzo AJ. Comparison of outcomes of prenatal versus postnatal presentation of posterior urethral valves: a systematic review and meta-analysis. World J Urol. 2022 Sep;40(9):2181-2194. doi: 10.1007/s00345-022-04097-x. Epub 2022 Aug 9. PMID: 35943527. [CrossRef] [PubMed]
- Wu CQ, Blum ES, Patil D, Shin HS, Smith EA. Predicting childhood chronic kidney disease severity in infants with posterior urethral valve: a critical analysis of creatinine values in the first year of life. Pediatr Nephrol. 2022 Jun;37(6):1339-1345. doi: 10.1007/s00467-021-05271-w. Epub 2021 Oct 30. PMID: 34716802. [CrossRef] [PubMed]
- McLeod DJ, Szymanski KM, Gong E, Granberg C, Reddy P, Sebastião Y, Fuchs M, Gargollo P, Whittam B, VanderBrink BA; Pediatric Urology Midwest Alliance (PUMA). Renal Replacement Therapy and Intermittent Catheterization Risk in Posterior Urethral Valves. Pediatrics. 2019 Mar;143(3):e20182656. doi: 10.1542/peds.2018-2656. Epub 2019 Feb 1. PMID: 30709926. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2026.10
|
| Cite this article as: | | Cardoso L, Santos P D, Stilwell R, Rodrigues C, Santos E, Forte J P, Morais P, Costa M, Borges M, Baptista R B, Francisco T, Neto G, Lima S, Silva A V, Vital V P, Cardoso D, Alves F, Abranches M. Kidney Outcomes in Children with Posterior Urethral Valves. Pediatr Oncall J. 2026;23. doi: 10.7199/ped.oncall.2026.10 |
|