Angela M Fagiana1, Daniel J Podberesky2, Kondi Wong3, Oluwole Fadare3, Christopher P Coppola4.
1Department of Pediatrics, Wilford Hall Medical Center, San Antonio, TX,
2Department of Radiology, Wilford Hall Medical Center, San Antonio, TX,
3Department of Pathology, Wilford Hall Medical Center, San Antonio, TX,
4Department of Surgery, Wilford Hall Medical Center, San Antonio, TX.
ADDRESS FOR CORRESPONDENCE
Christopher P Coppola, Section Chief, Pediatric Surgery, Wilford Hall Medical Center, 2200 Bergquist Av. Ste. 1 / MCSG. Lackland AFB, TX 78236. USA.
Email: ccoppola@pol.net | | Abstract | | A 13-year-old boy presented with a progressively enlarging right anterior axillary and chest wall mass. He first noted the mass three days after injuring his right shoulder while playing football. When the mass persisted, the possibility of hemorrhage into a soft tissue sarcoma in an adolescent was raised. Computed tomography and magnetic resonance imaging were used to evaluate the mass. Imaging revealed a multi-loculated cystic mass with an internal fluid-fluid level, and enhancement characteristics consistent with cystic lymphangioma and recent traumatic hemorrhage. This diagnosis was confirmed after histologic examination of the resected mass. This case illustrates an atypical adolescent presentation of cystic lymphangioma, manifest after trauma and masquerading as a soft tissue tumor. High resolution diagnostic imaging provided an accurate diagnosis and guided resection. | | | | Introduction | | Cystic lymphangiomas, once referred to as cystic hygromas, are congenital lymphatic malformations constituting 6% of all benign lesions of infancy and childhood. (1) Their origin is not completely understood, but it is thought that they occur if the primary lymphatic sacs fail to join the central venous system during embryologic development. (2) The sequestrations of lymphatic tissue form cysts that are composed of dilated endothelium lined channels. Most masses are identified by two years of age with approximately 50% noted at birth. (3) Approximately 75-90% are found in the head and neck, a region with a complex lymphatic system, with lesions also occurring in the axilla, mediastinum, chest wall, abdomen, inguinal region, and extremities.(3) Rapid or intermittent enlargement can occur secondary to infection or, as in the case presented here, injury related hemorrhage. | | | | Case Report | A 13-year-old boy with no significant past medical history presented with a progressively enlarging right axillary mass extending to the right chest wall. He had been playing football and fell onto his right shoulder. Three days later he noted the presence of a small pea-sized mass. Within five days the mass had increased in size to approximately 5 x 9cm. He reported having intermittent numbness and slight weakness in the right hand with use.
On initial physical exam, the patient was noted to have a soft, mobile, anterior axillary mass that was approximately 6 x 10cm and was nontender to palpation. His upper extremity strength was equal bilaterally and his sensation was intact. Bilateral radial pulses were normal.
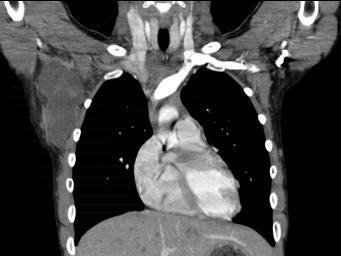
The mass was evaluated with computed tomography (CT) revealing a 9.6 (craniocaudad) x 4.4 (transverse) x 5.7 (anterior-posterior) cm multiloculated cystic mass within the upper right lateral chest wall and axilla, with very faint peripheral and septal enhancement most consistent with a large lymphatic malformation or cystic hygroma. (Figure 1a). The adjacent ribs, muscles, neurovascular structures and pleura were normal in appearance. Axial magnetic resonance imaging (MRI) revealed a multiloculated, multiseptated cystic mass with a distinct fluid-fluid level indicative of recent bleeding into the cyst. (Figure 1b). On post-gadolinium images, the mass demonstrated peripheral rim enhancement as well as enhancement of internal septations. (Figure 2). The MRI assisted in identifying the relationship of the mass to the subclavian vein and long thoracic and thoracodorsal nerves. A diagnosis of cystic lymphangioma was made based on imaging. Due to parents' and referring providers' concerns for a hidden malignancy and risk of future infection, elective resection after resolution of acute swelling was recommended.
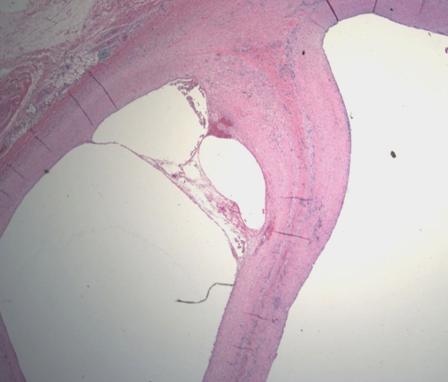
During the two weeks between presentation and elective operative resection, the mass decreased slightly in size and became more firm. The mass was entirely resected sparing the neurovasculature, and the patient did well postoperatively. The gross specimen was a large multiloculated cyst with serosanguinous fluid. (Figure 3). Histopathology was diagnostic for a lymphangioma. (Figure 4).
Figure 1: 1a: Coronal reformation from a contrast enhanced computed tomography scan demonstrates a cystic mass in the right axilla with faint rim and septal enhancement.
1b: Axial fat saturated fast spin echo T2 weighted magnetic resonance image demonstrates a multi-loculated cystic mass in the right lateral chest wall with internal fluid-fluid levels.
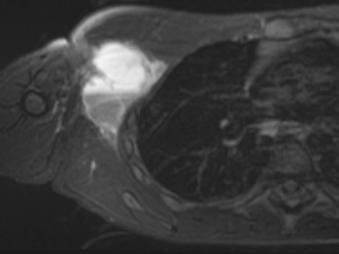
Figure 2: Axial (A) and coronal (B) fat saturated post-gadolinium T1 weighted images demonstrate circumferential rim enhancement of the mass, and enhancement of the internal septations of the mass. There is no enhancement of the internal cystic fluid.
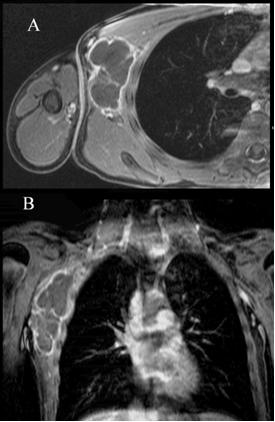
Figure 3: Resected specimen, axillary cystic lymphangioma (A) Cut surface of cystic lymphangioma (B)

Figure 4: Histologic sections showed large thin-walled cysts most of which were devoid of luminal contents and which were lined by variably attenuated endothelial cells.
 | | | | Discussion | Cystic lymphangiomas are benign lesions, but often involve extensive invasion of tissue planes by daughter cysts at the periphery of the primary cyst. (1) Treatment options include aspiration; injection with sclerosing agents, radiation and observation, but the most favored management option is surgical resection. Lymphangiomas recur after resection in as many as 10% of cases, and the recurrence rate after infection or repeat excision is even higher. (2) Because the most common cause of recurrence is inadequate tumor removal, a detailed delineation of the size and extent of the mass for successful surgical management is useful. (1) However, vital neurovascular structures should be spared since the lesion is not malignant. Sclerotherapy with OK-432 has given good results, but the highest success rate is still obtained with surgical excision. (5)
Typical MRI findings include high signal intensity and multiple cysts with well demarcated margins on T2-weighted images and low signal intensity on T1-weighted images. (1) Although the T1-weighted images usually demonstrate low signal intensity, the cyst may demonstrate mixed or even hyperintense signal depending on the age of the hemorrhage. (4) In this case, the MRI did reveal a heterogeneously hyperintense mass on T2-weighted images and a significant fluid-fluid level contained within the cyst with relatively more hypointense fluid layering posteriorly in the supine patient. On post-gadolinium T1-weighted imaging, cystic lymphangiomas typically show peripheral rim enhancement as well as enhancement of internal septations. The mass in this case was determined to be a large lymphatic malformation with associated internal hemorrhage.
As discussed, these lesions typically present prior to age 2 years. This child's presentation at age 13-years-old was atypical, but enlargement after injury in older patients has been reported. (6) Fung, et. al. described in their study that MRI produced highly detailed images that proved to be diagnostic and predictive of intraoperative findings, as was evident in this case. (1) Hemorrhage into the lymphatic malformation and the distinct appearance on MRI led to high confidence in the diagnosis and strategy of resection. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Fung K, Poenaru D, Soboleski DA, Kamal IM. Impact of magnetic resonance imaging on the surgical management of cystic hygromas. J Pediatr Surg. 1998; 33: 839-841. [CrossRef]
- Wever DJ, Heeg M, Mooyaart EL. Cystic hygroma of the shoulder region. A case report. Clin Orthop Relat Res. 1997; 338: 215-218. [CrossRef]
- Bloom DC, Perkins JA, Manning SC. Management of lymphatic malformations. Current Opinion Otolaryngol Head Neck Surg. 2004; 12: 500-504. [CrossRef]
- Cohen MD, DeRosa GP, Kleiman M, Passo M, Cory DA, Smith JA, et al. Magnetic resonance evaluation of disease of the soft tissues in children. Pediatrics. 1987; 79: 696-701. [PubMed]
- Okazaki T, Iwatani S, Yanai T, Kobayashi H, Kato Y, Marusasa T, et al. Treatment of lymphangioma in children: our experience of 128 cases. J Pediatr Surg. 2007; 42: 386-389. [CrossRef]
- Goh BK, Tan YM, Yap WM, Wong CY. Hemorrhage into a pancreatic lymphangioma after blunt trauma mimicking a post-traumatic pancreatic pseudocyst. J Trauma. 2006; 61: 992-994. [CrossRef]
|
| Cite this article as: | | Fagiana A M, Podberesky D J, Wong K, Fadare O, Coppola C P. An adolescent with an axillary mass. Pediatr Oncall J. 2009;6: 72-74. |
|