|
Short Stature - A skeletal dysplasia
Suksham Jain1, Parmanand Gupta2, Ravinder Kaur3.
1Department of Pediatrics, Government Medical College and Hospital, Chandigarh,
2Department of Orthopedics, Government Medical College and Hospital, Chandigarh,
3Department of Radio-diagnosis, Government Medical College and Hospital, Chandigarh.
ADDRESS FOR CORRESPONDENCE
Suksham Jain, Assistant Professor Pediatrics, Government Medical College and Hospital, Chandigarh. India.
Email: dr.sukshamj@gmail.com
|
|
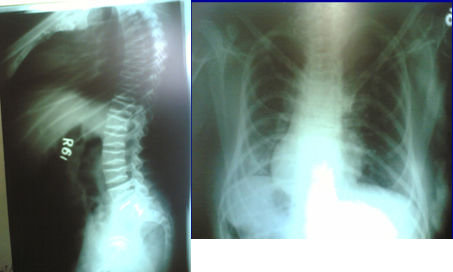
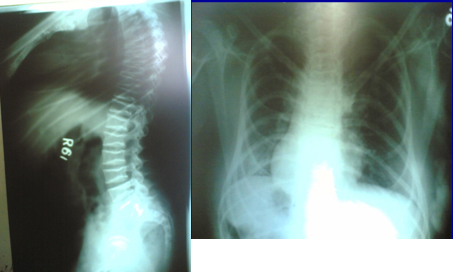
What is the diagnosis?
X-rays are suggestive of Mucopolysaccahroidosis, {MPS}. There was increase in urinary excretion of Heparin sulphate. The overall clinical scenario and biochemical markers were suggestive of MPS III {Sanfilippo disease}.
Mucopolysaccahropidosis type III is an autosomal recessive disorder, caused by deficiency in one of the four enzymes involved in the lysosomal degradation of the glycosaminoglycan- heparan sulphate. On the basis of enzyme deficiency there are four different biochemical subtypes, MPS III A, B, C and D with excessive excretion of Heparan sulphate in urine in all these types. Phenotype variations are less common in Sanfilippo than other types of MPS. A milder type may appear totally normal at birth. There is severe progressive central nervous system {CNS} involvement with mild somatic changes. Such disproportionate involvement of the CNS is unique of Sanfilippo. Delay in the diagnosis of MPS III usually occurs because of mild physical features, slow progression of severe CNS involvement and hyperactivity unlike other forms of MPS. Clinical course can be divided into three phases. First phase starts between 1 and 4 years, initially child is normal, later on there is developmental delay. Second phase starts around 3-4 years with severe behavior problems, progressive mental deterioration and dementia. In the third phase behavior problems decreases, there is motor retardation, spasticity and swallowing difficulties. Death usually occurs in 2-3 decade of life, although survival in the fourth decade has been reported {1}.
Presumptive diagnosis is on the basis of clinical and radiological features. Urine screening is done by Berry spot and Acid Turbidity tests. But screening tests may be falsely negative in Sanfillipo. Accurate and confirmed diagnosis is made by 2-dimensional electrophoresis, NMR spectroscopy {2}. Further quantitative estimation of Heparan sulphate can be done in urine. Other diagnostic tests are enzyme assay, which helps in carrier detection also. Amniotic fluid or chorionic villus biopsy can also be done for prenatal diagnosis in case of a positive family history {3}.
Authorship details: SK diagnosed the case` PG referred the case for the pediatric consultation and managed the skeletal deformities, RK diagnosed the skeletal deformities.
Conflict of Interest: None
Funding: Nil
REFERENCES
1. Valstar MJ, Ruijter GJ, van Diggelen OP, Poorthuis BJ, Wijburg FA. Sanfilippo syndrome: A mini-review. J Inherit Metab Dis. 2008 Apr 4. {Epub ahead of print}
2. Hochuli M, Wüthrich K, Steinmann B. Two-dimensional NMR spectroscopy of urinary glycosaminoglycans from patients with different mucopolysaccharidoses. NMR Biomed. 2003` 16: 224-236.
3. Whiteman P, Young E. The laboratory diagnosis of Sanfilippo disease. Clin Chim Acta. 1977` 76: 139-147.
Last Updated: 1st January 2010. Vol 7 Issue 1 Art # 6 |
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
|
|
|
| |
Cite this article as:
Jain S, Gupta P, Kaur R. Short Stature - A skeletal dysplasia. Pediatr Oncall J. 2010;7: 22-23.
|