Mark R. Corkins1, Kimberly E Applegate2, Karen West3.
1Division of Pediatric Gastroenterology, Riley Hospital for Children, Indiana Univ, Indianapolis, IN,
2Department of Radiology, Emory University, Atlanta, GA,
3Department of Surgery, Section of Pediatric Surgery, Riley Hospital for Children, Indiana Univ, Indianapolis, IN.
ADDRESS FOR CORRESPONDENCE
Mark R Corkins, Riley Hospital for Children, 702 Barnhill Drive, ROC 4210, Indianapolis, IN 46202. USA.
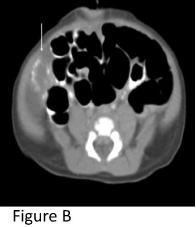
Email: mcorkins@iupui.edu | | Abstract | | A prenatal ultrasound at 28 weeks gestation demonstrated a heterogeneous mass in the inferior aspect of the liver. The infant was delivered at full term and had no clinical findings other than the palpable liver mass. All laboratory studies were normal. At 1 month of age, the patient underwent resection of the mass which represented an in utero ovarian torsion that had adhered to the liver. | | | | Keywords | | congenital liver mass | | | | Introduction | | Prenatal ultrasound has become a standard practice in obstetrical care. The technology of these devices has improved and therefore the ability of the ultrasound to detect a variety of anomalies before birth. The prenatal ultrasound can help guide preparation for anomalies that may require medical intervention but can also lead to parental anxiety when the findings are ambiguous. Finding a liver mass on a prenatal ultrasound raises a variety of diagnostic possibilities. There is a mixture of benign and malignant lesions that have a range of prognostic outcomes. | | | | Case Report | The patient was a day old female referred for evaluation of a liver mass. This mass was noted on a prenatal ultrasound at 28 weeks gestation. This mass was a 3.2 cm diameter cystic mass in the right side of the abdomen at the lower edge of the liver. After delivery, an ultrasound demonstrated a 4.4 x 3.4 x 4.8 cm multi-cystic mass at the inferior aspect of the right lobe of the liver (A). Laboratory studies showed normal clotting studies, liver functions and blood counts. Alpha fetal protein level was not excessive for age. The patient's examination was normal except for the palpable mass in the right upper quadrant of the abdomen. A subsequent CT scan showed similar findings and peripheral calcification in the lesion's wall (B). The patient fed well with excellent growth and at one month of age the patient underwent surgical resection. The liver lesion actually represented a case of ovarian torsion. In the operating room the patient was found to have an old torsion of the right ovary apparently due to an ovarian cyst. The torsed ovary was affixed to the lower aspect of the liver. The pathology confirmed the tissue to be ovarian.
Figure A: Ultrasound showing multi-cystic mass at inferior aspect of liver.

Figure B: CT scan showing peripheral calcification
 | | | | Discussion | The University of San Francisco Fetal Treatment center reviewed ten years of data for 1316 patients referred for congenital defects found on imaging (1). Sixteen had fetal tumors and only three were in the liver (1). The largest perinatal necropsy series covering 30 years and 17,417 infants found 46 tumors, including one hepatic adenoma and two liver hemangiomas (2). The most frequent liver tumors found in newborns are hepatoblastoma, hemangioendothelioma and mesenchymal hamartoma (3). Applegate and her colleagues reported a cystic liver lesion found during the third trimester of pregnancy on ultrasound that proved to be a hepatic adenoma (3). This lesion was in the anterior superior parenchyma of the right liver lobe. The vascular lesions of a congenital hemangioendothelioma has been described on prenatal ultrasound at 19 weeks gestation (4) and a giant hemangiomas has been described at 29 weeks gestation (5) both were associated with evidence of vascular shunting. A prenatal ultrasound of a hepatoblastoma has been reported at 36 weeks gestation with the description of a solid polylobular tumor in the right liver lobe with areas of hemorrhage, necrosis and small calcifications (6). In 2003, Kamata and his colleagues had tallied a total of 13 reported cases of prenatally detected mesenchymal hamartoma (7). These usually presented as a large, rapidly growing asymptomatic mass which in the majority of cases were cystic (7). These lesions may appear exophytic and it may be difficult to determine the organ of origin on pre-operative imaging.
The clue that this was an "extra-hepatic" mass was the finding that the mass appeared oval-shaped and contained many small cysts that are typical of ovarian follicles. The mass was cystic, free of blood flow on ultrasound, and contained a peripheral calcification that may be seen with infracted ovarian torsion. The size of the lesion varied very little from the time it was first found at 28 weeks gestation until delivery at full term. The completely normal laboratory studies also suggested that this might not be hepatic in origin. It is critical that investigation of neonatal cystic masses in girls include documentation of the normal ovaries in order to exclude this etiology in the differential diagnosis. Ovarian cysts in the newborn are commonly located in the abdomen due to the relatively small size of the pelvis and the long ovarian pedicle.
| | | | Financial Disclosure | | None | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest | | None | | |
- Sbragia L, Paek BW, Feldstein VA, Farrell JA, Harrison MR, Albanese CT, et al. Outcome of prenatally diagnosed solid fetal tumors. J Pediatr Surg 2001; 36: 1244-1247. [CrossRef]
- Werb P, Scurry J, Ostor A, Fortune D, Attwood H. Survey of congenital tumors in perinatal necropsies. Pathology 1992;24:247-253. [CrossRef]
- Applegate KE, Ghei M, Perez-Atayde AR. Prenatal detection of a solitary liver adenoma. Pediatr Radiol 1999;29:92-94. [CrossRef]
- Meirwitz NB, Guzman ER, Underberg-Davis SJ, Pellegrino JE, Vintzileos AM. Hepatic hemangioendothelioma: prenatal sonographic findings and evolution of the lesions. J Clin Ultrasound 2000;28(5):258-263. [CrossRef]
- Pott Bartsch E.M., Paek BW, Yoshizawa J, Goldstein RB, Ferrell LD, Coakley FV, et al. Giant fetal hepatic hemangioma. Case report and literature review. Fetal Diagn Ther 2003;18: 59-64. [CrossRef]
- Shih JC, Tsao PN, Huang SF, Yen BL, Lin JH, Lee CN, et al. Antenatal diagnosis of congenital hepatoblastoma in utero. Ultrasound Obstet Gynecol 2000;16: 94-97. [CrossRef]
- Kamata S, Nose K, Sawai T, Hasegawa T, Kuroda S, Sasaki T, et al. Fetal mesenchymal hamartoma of the liver: report of a case. J Pediatr Surg 2003;38:639-641. [CrossRef]
|
| Cite this article as: | | Corkins M R, Applegate K E, West K. A Congenital Liver Mass. Pediatr Oncall J. 2010;7: 44-45. |
|