Maryann Ugochi Ibekwe, Roland Chidi Ibekwe.
Department of Pediatrics, Ebonyi State University Teaching Hospital, Abakaliki, Ebonyi State, Nigeria.
ADDRESS FOR CORRESPONDENCE
Dr MaryAnn U Ibekwe, Department of Pediatrics, Ebonyi State University Teaching Hospital, Abakaliki, Ebonyi State, Nigeria.
Email: ugochiamadife@yahoo.com | | Abstract | Background:
Type 1 diabetes mellitus (DM) in the developing country remains under diagnosed and poorly managed. There is perennial unavailability of insulin, lack of trained manpower and government support.
Objective:
To audit the management of Type 1 diabetes in Ebonyi State University Teaching Hospital Abakaliki, South Eastern Nigeria before the advent of established Paediatric diabetic units.
Subjects and Methods:
It was a 9 years (1st January 2001- 31st December 2009) retrospective review of case files of children younger than 20 years with diagnosis of type 1 DM.
Results:
A total of 15,996 patients were seen during study period out of which 16 were diagnosed with type 1 DM, giving a case prevalence rate of 0.1/1000. The male to female ratio was 1:1.2. The mean age at presentation was 11.4 years. Average duration of illness before presentation at hospital was 7 weeks. The most prevalent presenting symptoms were dehydration 16 (100%), polyuria 15 (93.8%), and polydipsia 13 (81.3%). Fourteen (88%) patients first presented in the children's emergency room with Diabetic ketoacidosis (DKA), and the average duration of hospital stay when admitted was 43.8 days. Repeated DKA and hypoglycemia was reported in 25% of the patients. Eighteen percent of patients opted for discharge against medical advice (DAMA) while about 70% were lost to follow up.
Conclusion:
Diabetic management over the past 10 years in this hospital is suboptimal with very poor outcomes. Lack of trained manpower, poverty and ignorance are significant contributory factors to the poor management outcome and high default rate. | | | | Introduction | Type 1 Diabetes Mellitus (DM) in the developing country remains under diagnosed and poorly managed. With the high contribution of malnutrition, infections and infestation to childhood morbidity and mortality in sub Saharan Africa, there is scant interest in non-communicable diseases. (1,2) There is however, an emerging evidence of increasing prevalence of non-communicable diseases of which Type 1 DM is a major one. (3) The few published reports on type 1 DM from Africa highlighted two major issues which are that it is under diagnosed and there is unavailability of insulin. (3,6-8). The former is largely a result of lack of trained manpower especially trained pediatric endocrinologist and diabetic nurses, as well as lack of established pediatric diabetic clinics. The latter is due to low purchasing power of the patients in buying insulin as well as poor government support in the procurement and distribution of insulin. The morbidity and mortality of Type 1 DM in Nigeria is very high. (3,6,7) and the governments are not prepared to take this as a high priority in the National health care agenda as they are still burdened with tackling HIV/AIDS, malaria and currently polio eradication.
There is paucity of information on prevalence and outcome of type 1 DM in Nigeria and no published data from Abakaliki. Most of the few published works focused more on type 2 DM. Type 1 DM were managed by general practitioners, adult physicians and pediatricians without specialised training in paediatric endocrinology. In most cases, there are no standard practices for managing children presenting with DM.
This communication attempts to audit the management of Type 1 DM in Ebonyi State University Teaching Hospital, Abakaliki, South Eastern Nigeria. Abakaliki is located in the south-eastern part of Nigeria, covering an area of approximately 51km 2. It has an estimated population of 255,000 people who are predominantly small to medium-scale farmers, civil servants, and traders. During the period under review, the hospital did not have any pediatric endocrinologist and there was no diabetic clinic. Children with Type 1 DM were managed by general pediatricians.
| | | | Methods & Materials | | The study involved a 9 years (1st January 2001-31st December 2009) retrospective review of case files of children younger than 20 years with diagnosis of Type 1 DM. Age, sex, presenting features, insulin management, complications and outcome of patients were extracted from the hospital records. | | | | Discussion | In this study, the prevalence of Type 1 diabetes in EBSUTH, Abakaliki is 0.1/1000, which is lower than the 3.1/1000 reported by Adeleke et al (7) in a similar hospital based study in Kano, North Western Nigeria. This finding can be criticized that it may not be representative of the actual population prevalence on account of this being a hospital based retrospective data, with all its limitations. The diagnosis of Type 1 DM may have been missed in the hospital or children may have already died before they reached the hospital. Our finding is however similar to Afoke et al of 0.33/1000 of Type 1 DM among children in Ishiellu, a community close to the study center. (9) This low prevalence is also in keeping with the few epidemiological studies on type 1 DM in African children, for instance Tanzania was estimated to have a prevalence of 1.5/100,000 (10) and Sudan 10.3/100,000 (11). This low prevalence had been postulated to be due to reduced genetic susceptibility to DM among black African, a finding also observed among Black Americans. (12,13) The other contributory factor could be the high mortality among African children with type 1 DM, in rural Mozambique life expectancy was reported to be as low as 0.6 years. (8)
In most of the reports, the prevalence of type 1 DM was found to increase with increasing age, (3,6,14) this is also our finding. The study revealed that 87% of the patients were above the age of 8 years at the onset of the disease. In fact Bella et al (6) reported that insulin dependent diabetics in Nigerian Africans rarely occurred in patients younger than 10 years. A female preponderance, was noted in studies from other parts of Nigeria, Ethiopia and Sudan. (3,6,7,14,15) The reason for this is not clear. Bella et al however, postulated that it could be due to the presence of HLAB8/DR3 haplotype which is more common among females, and is an auto immune disorder that is associated with other endocrinopathies and pancreatic islet cell antibodies. (6) This theory is negated by the absence of HLAB8 and pancreatic islet cell antibody among Nigerian diabetic patients studied by Oli and co-workers. (16)
Most of the patients presented rather late as more than half of the patients delayed for more than 3 weeks before presenting to the hospital. The late presentation may be the cause of the high incidence of DKA seen in 88% of all newly diagnosed diabetics. This is not surprising in a population where there is lack of awareness of symptoms and signs of Type 1 DM in children coupled with intercurrent infections, poverty and strong traditional beliefs. Other studies in Africa reported similar late presentation of type 1 DM in children. (3,5,7) The virtual lack of trained health care professionals in diabetic management could have undermined early detection and optimal management of diabetes in this center as in most of sub-Saharan Africa. (3,8,10,11) The study in Tanzania highlighted the relationship between late presentation and a high incidence of diabetics presenting as DKA. (11)
Management of these patients was not optimal as shown by the slow rate of achieving glycemic control, prolonged hospital stay, and the fact that dosing of insulin and glycemic control both during the acute phase of DKA and maintenance phase falls short of the standard practices in Type 1 DM management in children. This study highlights some of the challenges in managing Type 1 DM in Abakaliki, this include extreme poverty, in a country where more than 60% of the population live below the poverty line of 1$ per day. Diagnosis of Type 1 DM is almost a death sentence, in Nigeria. Treatment of diabetes is not free, most of the patients could not afford the cost of insulin, investigations and regular clinic visits, and this is worsened by the well known perennial lack of and inaccessibility of insulin. (6-8) Ignorance is also a major impediment to optimal care, most of the families are poorly educated with deep rooted traditional beliefs, this accounts for late presentation, use of herbal medication, poor compliance to prescribed medications, high rate of discharge against medical advice (DAMA) and also high default rate. The other major challenge was the absence of trained manpower, during the period under review there was no trained pediatric endocrinologists, no pediatric diabetic clinic, no diabetic nurse or dietician, there was no established protocol for managing type 1 DM and DKA, and this is responsible for the inconsistent management schedule for both DKA and type 1 DM. Also noted in this review is the very high rate of DAMA and loss to follow up. It is a common practice in our community that parents or guardian opt to discharge their wards against medical advice and do not keep clinic appointments. This is mainly due to frustration and inability to meet the financial cost of treatment. The underlining issue is ignorance, poverty and poor standard of care as highlighted by Ibekwe et al. (18) This problem makes management of diabetics very frustrating; they fail to honour hospital appointment, only for the child to represent either with DKA or hypoglycemia. This explains the high rate of repeated DKA and hypoglycaemia among the patients. It also makes it difficult to reliably conclude on the absence of mortality observed in this study; some of the children may have died at home or elsewhere.
| | | | Conclusion | | Diabetic management over the past 10 years in EBSUTH Abakaliki is suboptimal with very poor outcomes. There is need to institute measures for early diagnosis of type 1 DM, through awareness campaign to both the public and healthcare providers in Nigeria. Health care workers should be trained to recognize and treat type 1 DM and the centers should set up a comprehensive diabetic programme, including a standard protocol for management of DKA. Free blood glucose meters, strips and insulin are needed. There is need for government to either provide health insurance or provide free treatment for children with chronic conditions like type 1 DM; Health education of the populace could increase the awareness about type 1 DM because the observed low prevalence may not be real. | | | | Results | Demographic data
The total number of pediatric patients admitted to the hospital during the study period was 15,996. Sixteen out of these patients were diagnosed with Type 1 DM, giving a case prevalence rate of 0.1/1000. Table 1 shows the age and sex distribution of patients. The male to female ratio was 1:1.2. The mean age at presentation was 11.4 years. However, 87.5% of the patients were aged > 8 years.
Table 1: Age and sex distribution of children with Type 1 DM
| Age |
1-4 |
5-9 |
10-14 |
15-19 |
Total |
| Male |
0 |
3 |
1 |
1 |
5 |
| Female |
1 |
1 |
6 |
3 |
11 |
| Total |
1 |
4 |
7 |
4 |
16 |
Clinical Presentations
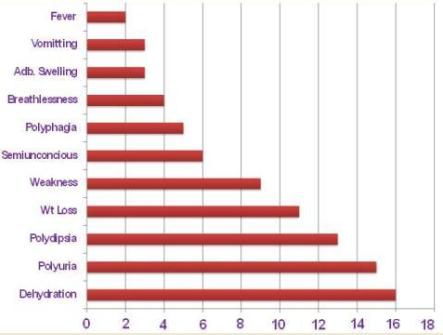
Duration of symptoms before presentation at the hospital was 2 weeks for 7 (44%) patients, 3-6 weeks for 5 (31%) patients, 3-6 months for 3 (19%) patients and more than 6 months for 1(6%) patient. The most prevalent presenting features were dehydration in 16 (100%) patients, followed by polyuria in 15 (93.8%), polydipsia in 13 (81.3%) and weight loss in 11(68.8%). Other clinical features are depicted in Figure 1. Fourteen (88%) of the 16 patients presented in Diabetic Ketoacidosis (DKA). Three (18.8%) patients had used herbal medicine before presenting, while 4 (25%) where referred from a peripheral hospital.
Figure 1: Clinical Presentations of Patients with Diabetes Mellitus
Hospital management
Table 2 highlights the mean distribution of blood sugar results and duration of hospital stay.
Table 2: Blood sugar values and Duration of hospital stay
| Variables |
n |
Mean |
Range |
| Initial blood sugar (mg/dl) |
16 |
493 |
294-800 |
| Average random blood sugar 48 hrs post admission (mg/dl) |
14 |
409.5 |
217-995 |
| Average random blood sugar 1 week post admission (mg/dl) |
13 |
370.1 |
176-698 |
| Number of blood sugar measure/ day |
15 |
1.4 |
1-4 |
| Duration of hospital stay |
15 |
43.87 |
4-60 |
Intravenous rehydration was given to 15 (93%) of the patients. Only 3 (18%) of the patients could measure their blood glucose at least twice a day while on admission. The average number of times blood sugar was measured in a day in these patients was 1.4 times with a range of 1-4 times. Eleven (75%) of the patients received IV regular short-acting insulin during the initial insulin management of DKA. Three (19%) patients were managed using sliding scale while one patient was placed on insulin lente and dietary restriction. Short-acting regular insulin was used in half (50%) of the patients during the maintenance phase, while 4 (25%) were on pre mix insulin, 3 (18%) of patients were placed on lente insulin only and one patient received glucophage during maintenance period. The most common complications were repeated DKA and hypoglycemia in 4 (25%) of the patients each. Two (12.5%) patients had protein energy malnutrition while one patient had nephropathy.
Three (18%) patients opted for discharge against medical advice (DAMA) while about 70% of the patients were lost to follow up. There was no record of death. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Childhood mortality Coordination Group. Tracking progress towards the Millennium Development Goals reaching consensus on child mortality levels and trends. Bull WHO 2006; 84: 225-232. [PubMed] [PMC free article]
- Black RE, Moris SS, Bryce J. Where and why are 10 million children dying every year- Lancet 2003; 361: 2226 - 2234.
- Edna SM, Elusiyan JE, Adesiyun OO et al. Type 1 diabetes in the African population: epidemiology and management challenges. Acta Biomed. 2008; 79: 255-259.
- Mario A, Sridevi A. Diabetes in Sub - Saharan Africa: Kenya, Mali, Mozambique, Nigeria, South Africa and Zambia. Int J Diabetes Dev Ctries. 2008; 28: 101-108. [CrossRef]
- Levitt NS. Diabetes in Africa: epidemiology, management and healthcare challenge. Hearts 2008;94: 1376 - 82. [CrossRef]
- Bella AF. A prospective study of insulin dependent diabetic Nigerian Africans. J Natl Med Assoc. 1992; 84: 126-128. [PubMed] [PMC free article]
- Adeleke SI, Asani MO, Belonwu RO, et al Childhood diabetes mellitus in Kano, NorthWest, Nigeria. Nig J Med. 2010; 19: 145-147. [CrossRef]
- Beran D, Yudkin JS, de Courten M. Access to care for patients with insulin requiring diabetes in developing countries case studies of Mozambique and Zambia. Diabetes Care. 2005; 28: 2136-2140. [CrossRef]
- Afoke AO, Ejeh NM, Nwonu EN, Okafor CO, Udeh NJ, Ludvigsson J. Prevalence and clinical picture of IDDM in Nigerian Igbo school children. Diabetes Care. 1992; 15: 1310 - 1312. [CrossRef]
- Swai AB, Lutale JL, McLarty DG. Prospective study of incidence of juvenile diabetes mellitus over 10 years in Dar es Salaam, Tanzania. BMJ. 1993; 306: 1570-1572. [CrossRef]
- Elamin A, Omer MI, Zein K, Tuvemo T. Epidemiology of childhood type 1 diabetes in Sudan, 1987-1990. Diabetes Care. 1992; 15: 1556-1559. [CrossRef]
- MacDonald MJ. Lower frequency of diabetes among hospitalized Negro than white children. Theoretical implications. Acta Genet Med Gamelol. 1974; 24: 119 -126.
- Lorenzi M, Cogliero E, Schmidt NJ. Racial differences in incidence of juvenile onset type 1 diabetes: Epidemiologic studies in southern California. Diabetologia 1985;28: 734 -8. [PubMed]
- Kalk WJ, Huddle KR, Real FJ. The age of onset and sex distribution of insulin-dependent diabetes mellitus in Africans in South Africa. Postgrad Med J 1993;69: 552-6. [CrossRef]
- Motala AA, Omar MAK, Pirie FJ. Epidemiology of type1 diabetes in Africa. J Cardiovasc Risk. 2003; 10: 77-83. [CrossRef]
- Oli JM, Bottazo GF, Doniach LB. Islet cell antibodies in Nigerian Diabetes. Lancet 1980; 1: 1090. [CrossRef]
- Ibekwe RC, Muoneke VU, Nnebe-Agumadu UH, Amadife MU. Factors influencing discharge against medical advice among paediatric patients in Abakaliki Southeastern Nigeria. J Trop Pediatr. 2009; 55: 39-41. [CrossRef]
|
| Cite this article as: | | Ibekwe M U, Ibekwe R C. Pattern of Type 1 Diabetes Mellitus in Abakaliki, Southeastern, Nigeria. Pediatr Oncall J. 2011;8: 59-62. |
|