|
Recurrent respiratory tract infections in an infant
Anupama Agrawal, Kirandeep Sodhi, Sanjiv Kakkar.
Department of Pediatrics, Command Hospital, Central command, Lucknow, India.
ADDRESS FOR CORRESPONDENCE
Col {Mrs} Kirandeep Sodhi, Sr Adv Pediatrics, Department of Pediatrics, Command Hospital, Central command, Lucknow 226002, India.
Email: sodhikirandeep@gmail.com
|
|
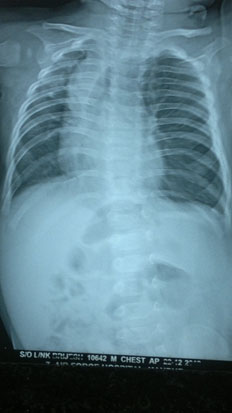
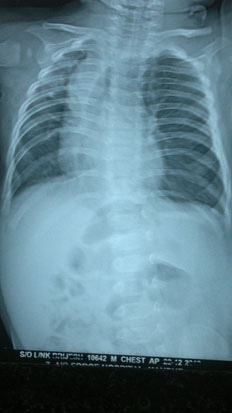
What is the diagnosis?
Congenital lobar emphysema {CLE}. X-Ray chest of the infant shows volume loss left lung with mediastinal shift to the right suggestive of congenital lobar emphysema. CLE is a rare congenital malformation of lung development with a prevalence of 1 in 20,000 to 1 in 30,000. {1} It occurs when partial bronchial obstruction causes hyperinflation of the lung lobe which in turn compresses the normal lung parenchyma causing contralateral mediastinal shift. {2} The causes of the bronchial obstruction can be multifactorial. In 50 percent of cases there is decrease in the bronchial cartilage tissue producing a ball valve effect with consequent overinflation. In the rest of the cases bronchial obstruction may be due to vascular abnormalities, bronchial stenosis, bronchogenic cysts or endobronchial obstruction due to viscid secretions, mucus plugs or granulation tissue. {3} A chest radiograph helps in the diagnosis but is not definitive. The characteristic appearance is that of pressure expansion of a lobe of lung causing compression of adjacent lobes. The mediastinum may be displaced away from the emphysematous side. In severe cases the over expanded lung may be herniated into the contralateral hemithorax. {4} A CT scan confirms the diagnosis and may rule out associated anomalous vascular slings. The most commonly accepted form of treatment is surgical removal of the affected lobe. However conservative management may be considered in those patients with mild disease who have no respiratory distress and are able to feed and grow. {5}
Last Updated: Dec 2013 Vol 10 Issue 12 Art # 65 |
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
|
- Thakral CL, Maji DC, Sajwani MJ. Congenital lobar emphysema: Experience with 21 cases. Pediatr Surg Int. 2001; 17: 88-91 [CrossRef] [PubMed]
- Datta AK, Mandal S, Jana JK. Congenital lobar emphysema – A case report. Cases Journal. 2009; 2: 67 [CrossRef] [PubMed] [PMC free article]
- Doull IJ, Connett GJ, Wamer JO. Bronchoscopic appearances of congenital lobar emphysema. Pediatr Pulmonol. 1996; 21: 195-197 [CrossRef]
- Biswal N, Mathai B, Bhatia BD, Bhat BV, Puri RK, Karthikayan G et al. Congenital lobar emphysema. Indian Pediatr. 1993; 30: 1349-1354 [PubMed]
- Mei-Zahav M, Konen O, Manson D, Langer JC. Is congenital lobar emphysema a surgical disease? Journal Pediatr Surg. 2006; 41: 1058-1061 [CrossRef] [PubMed]
|
|
DOI: https://doi.org/10.7199/ped.oncall.2013.65 |
| |
Cite this article as:
Agrawal A, Sodhi K, Kakkar S. Recurrent respiratory tract infections in an infant. Pediatr Oncall J. 2013;10: 125. doi: 10.7199/ped.oncall.2013.65
|