Amber Healy1, Divine Ribakare2, Jeffrey Benseler1, Jay Shubrook3.
1Department of Specialty Medicine, Ohio University Heritage College of Osteopathic Medicine, Athens, Ohio, USA,
2OMS-4 Ohio University Heritage College of Osteopathic Medicine, Athens, Ohio, USA,
3Department of Family Medicine, Ohio University Heritage College of Osteopathic Medicine, Athens, Ohio, USA.
ADDRESS FOR CORRESPONDENCE
Amber Healy, DO, 105 Parks Hall OU-HCOM Department of Specialty Medicine, Athens, Ohio, 45701.
Email: holdera@ohio.edu | | Keywords | | histoplasmosis, diabetes, immunocompetent | | | An 11-year-old female with a past medical history of well-controlled type 1 diabetes (T1DM) with glycosylated hemoglobin (HbA1c) of 7.2% presented with recurrent fever and cough for 3 weeks. During this time she had visited an urgent care setting 3 times and been treated for upper respiratory infection, otitis media, and bronchitis without relief of symptoms. At a follow-up outpatient visit, a chest X-ray revealed a pneumonia in the left upper lung for which she was treated with another course of antibiotics to cover atypical pathogens. Over the next few days the patient's chest pain worsened and she developed nausea and vomiting where she was only able to tolerate liquids. She also developed a rash on her lower legs that was not itchy or painful. She denied any sick contacts, recent travel, exposure to tuberculosis, hiking, or camping. Throughout this course she had two negative streptococcal throat swabs. Laboratory tests at this visit showed an ESR of 111 mm at end of 1 hour, white blood cells (WBC) 12,600/cumm with a normal differential, hemoglobin of 11.4gm/dl and a hematocrit of 33.2, as well as elevated platelets at 469,000 cells/cumm. She was started on ceftriaxone and transferred to a pediatric tertiary care center.
Upon admission repeat work-up was consistent with a community acquired pneumonia that had not been sufficiently treated. Blood and urine cultures were obtained and she was started on the combination of ampicillin-sulbactam and azithromycin. She continued to have fevers and cough as well as decreased appetite and fatigue despite this therapy. Three days after admission the patient began to complain of left upper quadrant abdominal pain. WBC was 16,700/cumm, ESR was 50 mm at end of 1 hour, and C-reactive protein (CRP) was 5.6. An abdominal ultrasound showed borderline splenomegaly with multiple small round lesions suggestive of abscesses.
The infectious disease team was consulted and recommended the following tests: Bartonella titers, fungal antibody panel, Epstein Barr Virus titers, purified protein derivative, acid-fast bacillus stain, Mycoplasma antibody, rhinovirus and enterovirus PCR. All of these lab results were negative except for rhinovirus. Histoplasmosis was suspected based on negative lab work, splenomegaly, and the patient living in an endemic area.
The patient was tested for histoplasma antigen and started on Amphotericin B liposome. The urine histoplasma antigen was negative but her panel of fungal antibodies was strongly positive for histoplasma.
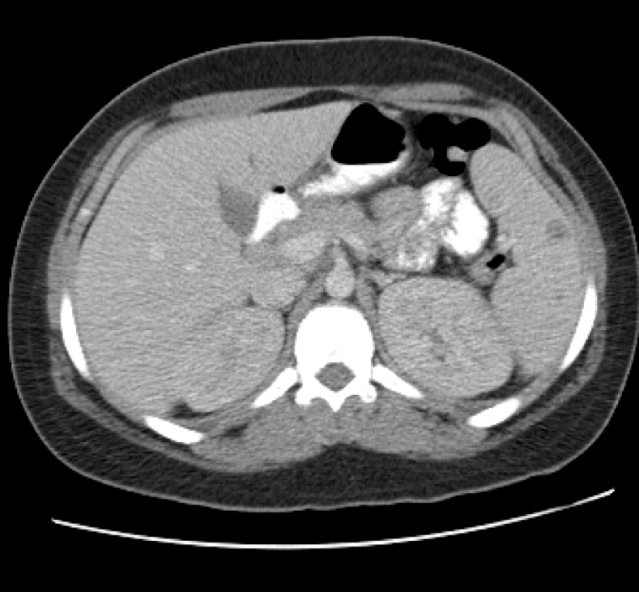
A CT scan showed a large subcarinal mass and left upper lobe airspace disease. (Figure 1)
Figure 1: CT showing one of multiple small splenic abscesses.
At this point she was started on itraconazole. After 2 weeks in the hospital she was much improved and was discharged on a 2 week outpatient course of itraconazole.
Histoplasmosis is common in the Ohio River Valley, where up to 80% of the population would test positive via skin tests. (1) Histoplasmosis is usually asymptomatic and self-limiting in immunocompetent patients. (2) It is possible that the patient's underlying T1DM had affected this patient's cellular immunity (3) making her more susceptible to this infection and dissemination with both pulmonary and splenic involvement. Risk factors for disseminated histoplasmosis include: HIV/AIDS, solid organ transplant, immunosuppressive medications, immunosuppressive disorders, and age. (2) There are isolated case reports of T1DM and disseminated histoplasmosis. (2,4,5-7) Patients with diabetes mellitus are more susceptible to infections compared to those without diabetes mellitus. Immunologic studies have demonstrated defects in the host immune mechanism in diabetics. Phagocytic capabilities of diabetics of polymorphonuclear leukocytes (PMN) are affected by the hyperglycemic state in rat models. The defects include: impaired migration, intracellular cellular killing, and chemotaxis, which are thought to be due to decrease membrane fluidity. (8)
Disseminated histoplasmosis infections are unusual even in immunosuppressed individuals. It is even rarer in an immunocompetent patient, like the patient presented here. Histoplasmosis should, still be considered in the differential in individuals who present with persistent and unusual symptoms in endemic areas. T1DM may also play a role in altering immune function leading to susceptibility of such an infection as demonstrated in this case. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Department of Health and Human Services Centers for Disease Control and Prevention (National Institute for Occupational Safety and Health). Histoplasmosis: protecting workers at risk. DHHS (NIOSH) Publication 97-146, September 1997.
- Kadaria D, Muthiah MP, Sinclair SE. Unusual presentations of disseminated histoplasmosis. Tenn Med. 2012; 105: 39-40. [PubMed]
- Wheat LJ, Slama TG, Norton JA, Kohler RB, Eitzen HE, French ML, et al. Risk factors for disseminated or fatal histoplasmosis. Ann Intern Med. 1982; 96: 159-63. [CrossRef] [PubMed]
- Chan KS, Looi LM, Chan SP. Disseminated histoplasmosis mimicking miliary tuberculosis: A case report. Malaysian J Pathol. 1993; 15: 55-158.
- Smith GD, Shatford RA. Histoplasmosis infection presenting as an isolated subcutaneous periarticular upper limb swelling in the immunosuppressed patient. J Hand Surg. 2005; 30: 229-232. [CrossRef] [PubMed]
- Ralph AF, Raines M, Rode JW, Currie BJ. Histoplasmosis in two aboriginal patients from Australia's tropical northern territory. Trans R Soc Trop Med Hyg. 2006; 100: 888-90. [CrossRef] [PubMed]
- Corcho-Berdugo A, Munoz-Hernandez B, Palma-Cortes G, Ramírez-Hernandez A, Martínez-Rivera M, Frias-de Leon M, et al. An unusual outbreak of histoplasmosis in residents of the state of Mexico. Gaceta Medica de Mexico. 2011; 47:377-384.
- Diabetes in America. 2nd ed. Washington: National Diabetes Data Group, National Institute of Diabetes and Digestive and Kidney Diseases, National Institute of Health, 1995.
DOI: https://doi.org/10.7199/ped.oncall.2014.8
|
| Cite this article as: | | Healy A, Ribakare D, Benseler J, Shubrook J. DISSEMINATED HISTOPLASMOSIS IN AN 11 YEAR OLD FEMALE WITH TYPE 1 DIABETES. Pediatr Oncall J. 2014;11: 23-24. doi: 10.7199/ped.oncall.2014.8 |
|