Anupama Aggarwal, VR Sinha, Kirandeep Sodhi, Sanjiv Kakkar, Ashwini Kumar.
Department of Pediatrics, Command Hospital, Central command, Lucknow, India.
ADDRESS FOR CORRESPONDENCE
Col (Mrs) Kirandeep Sodhi, Sr Adv Pediatrics, Department of Pediatrics, Command Hospital, Central command, Lucknow 226002, India.
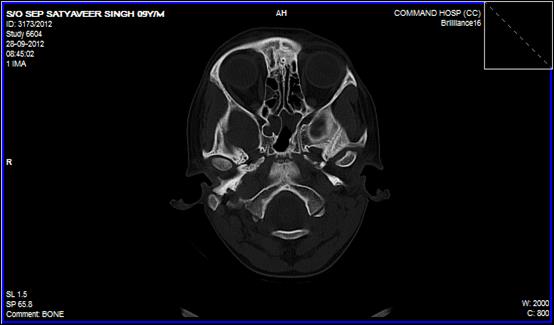
Email: sodhikirandeep@gmail.com | A 10 years old boy presented with complaints of fever, vomiting, headache and altered sensorium for one day. There were no seizures. He had similar complaints twice before in the last two and a half years necessitating hospitalisation and intravenous antibiotics. Detailed reports of only one such episode were available when the Cerebrospinal fluid (CSF) examination had neutrophilic leucocytosis, increased proteins and decreased sugar. During the second episode, he was also administered anti-tuberculous therapy (ATT) for six months, although the rationale of starting the same was not clear. On further probing, the mother recalled the child had a head injury after a fall three years ago. Examination revealed a febrile child with altered sensorium (Glasgow coma scale 13/15). He had marked photophobia, neck rigidity without focal neurological deficit. Examination of the spine, ears and nose were normal. Laboratory investigations revealed a neutrophilic leucocytosis and elevated C - reactive protein (CRP). CSF examination revealed neutrophilic pleocytosis, low sugars and increased proteins suggestive of a pyogenic process. Gram’s stain was negative. CSF culture did not show any growth. X-ray paranasal sinus was normal. Cranial CT scan showed a defect in the right cribriform plate. (Figure 1). Patient was treated with Inj ceftriaxone and vancomycin for a period of 21 days. The patient recovered completely. Thereafter he was taken up for an endoscopic duroplasty by the ENT colleagues. The patient is under regular follow up, is doing well and is asymptomatic.
Figure 1: Cranial CT scan showed a defect in the right cribriform plate
Recurrent meningitis indicates pyogenic meningitis occurring on two or more occasions after an intervening period of full convalescence. (1) It is defined as two or more episodes of meningitis caused by a different bacterial organism or, alternatively, a second or further episode caused by the same organism with a greater-than-3-week interval after the completion of therapy for the initial episode. (2,3) Recurrent meningitis in childhood should always prompt a search for an underlying cause as it is usually associated with a predisposing factor. Recurrent attacks of bacterial meningitis usually follow in the wake of cranial trauma. Other causes can be sinusitis, mastoiditis, congenital dermal sinuses and immunological causes related to humoral immunity and the complement system or intracranial dermoids. (4) When CSF communicates with the middle ear cavity, nose or nasopharynx, there is potential for CSF bacterial contamination and meningitis. Investigation of patients with recurrent bacterial meningitis should include a complete history, stressing any previous head trauma including that which may have been sustained several years before the onset of first episode of meningitis, a history of frequent or chronic middle ear infection, surgery on the ear, nose and paranasal sinuses. A meticulous examination of the head and spine for fistulous tracts or cutaneous stigmata should be done in these patients to pick up occult spinal defects. An immune screen may also be carried out. (5)
Most acute post-traumatic cases of CSF rhinorrhoea resolve with conservative treatment. In the event of a chronic or prolonged leak, however, a surgical solution is mandatory. With improvements in technology and instrumentation in the last decade, the surgical repair of CSF leak has evolved into an endoscopy based procedure from the one based on craniotomy in the past. Studies of large series of endoscopically treated patients report high success rates, approaching 95% at the first closure attempt. (6) | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Al Zamil F. Recurrent bacterial meningitis: report of two cases from Riyadh, Saudi Arabia. Ann Trop Paediatr. 1999; 19: 395-399. [CrossRef] [PubMed]
- Drummond DS, de jong AL, Giannoni C, Sulek M, Friedman EM. Recurrent meningitis in the paediatric patient-the otolaryngologist's role. Int J Pediatr Otorhinolaryngol. 1999; 48: 99-208. [CrossRef]
- Bell BE. Recurrent meningitis in children. Pediatr Neurol. 1992; 39: 651-668.
- Harter DH. Bacterial meningitis and brain abscess. In: Harrison's. Principles of Internal Medicine, 12th edn. Eds. Isselbacher KJ, Brainwald E, Wilson JD, et al. New York, McCraw Hill. 1991: 2023-2030.
- Thong YH, Simpson DA, Muller Eberhard HJ. Homozygous deficiency of the second component of complement presenting with recurrent bacterial meningitis. Arch Dis Child. 1980,55: 471-473. [CrossRef] [PubMed]
- Gilat H, Rappaport Z, Yaniv E. Endoscopic Transnasal Cerebrospinal Fluid Leak Repair: A 10 Year Experience. Isr Med Assoc J. 2011; 13: 597-600. [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2014.25
|
| Cite this article as: | | Aggarwal A, Sinha V, Sodhi K, Kakkar S, Kumar A. Recurrent Meningitis in a Child. Pediatr Oncall J. 2014;11: 55. doi: 10.7199/ped.oncall.2014.25 |
|