|
MASS IN NASAL CAVITY
Jahangeer Ahmad Bhat, Owais Tantry, Mir Rizwan, Hanan Madni.
Department of Radio-diagnosis, Government Medical College, Srinagar, Jammu and Kashmir, India.
ADDRESS FOR CORRESPONDENCE
Dr Jahangeer Ahmad Bhat, Senior Resident, Govt Medical College, Srinagar, India.
Email: drjahangeerahmadbhat@yahoo.com
|
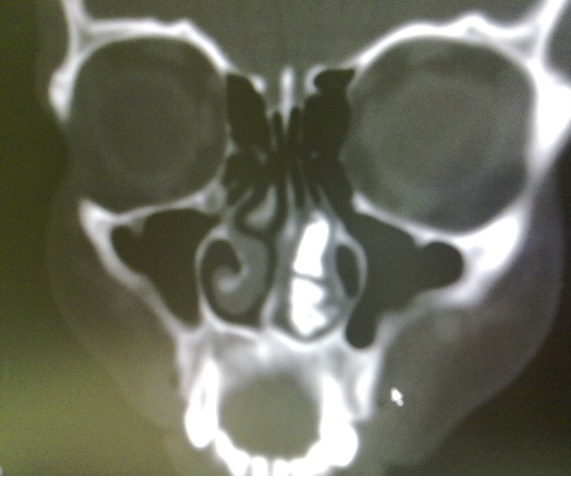
What is the diagnosis?
Ectopic supernumerary teeth is a rare condition and there are multiple causes of ectopic eruption of teeth e.g., developmental disorders like cleft palate, facial trauma, maxillary infection, cyst, crowding, genetic factors and high bone density. {1,2} Ectopic teeth may be permanent, deciduous, and supernumerary. Imaging helps in making proper diagnosis and planning treatment. The incidence of supernumerary teeth is 0.1–1 percent in general population. {3} The most common location is the upper incisor area, known as mesiodens. The extra teeth have an atypical crown, and they may be in a vertical, horizontal, or inverted position. They may grow into the nasal cavity. The teeth may be asymptomatic or cause a variety of signs and symptoms, including facial pain, nasal obstruction, headache, epistaxis, foul-smelling rhinorrhea, external nasal deformities, and nasolacrimal duct obstruction. {4,5} Supernumerary teeth develop either from a third tooth bed that arises from the dental lamina near the permanent tooth bud or, possibly, from splitting of the permanent bud itself. {3} Another theory is that their development is a reversion to the dentition of extinct primates, which had three pairs of incisors. {3} The diagnosis of nasal teeth is made on the basis of clinical and radiographic findings. Clinically, an intranasal tooth may be seen as a white mass in the nasal cavity surrounded by granulation tissue and debris. {4} Radiographically, the nasal teeth in our patient appeared as radiopaque lesions with the same attenuation as that of the oral teeth. With the bone window setting, the central radiolucency, which is correlated with the pulp cavity, may have a spot or slit, depending on the orientation of the teeth. The soft tissue surrounding the radiopaque lesion is consistent with granulation tissue found on clinical and pathologic examinations. The differential diagnosis of nasal teeth includes radiopaque foreign body` rhinolith` inflammatory lesions due to syphilis, tuberculosis, or fungal infection with calcification` benign tumors, including hemangioma, osteoma, calcified polyps, enchondroma, and dermoid` and malignant tumors, such as chondrosarcoma and osteosarcoma. However, the CT findings of tooth-equivalent attenuation and a centrally located cavity are highly discriminating features that help to confirm the diagnosis. Removal of nasal teeth is generally advocated to alleviate the symptoms and prevent complications. |
- Carver DD, Peterson S, Owens T. Intranasal teeth: a case report. Oral Surg Oral Med Oral Pathol. 1990; 70: 804-805 [CrossRef]
- Smith RA, Gordon NC, De Luchi SF. Intranasal Teeth. Report of two cases and review of the literature. Oral Surg Oral Med Oral Pathol. 1979; 47: 120-122 [CrossRef]
- Thawley SE, Ferriere KA. Supernumerary nasal tooth. Laryngoscope 1977;87:1770–1773 [CrossRef] [PubMed]
- Smith RA, Gordon NC, De Luchi SF. Intranasal teeth: report of two cases and review of the literature. Oral Surg Oral Med Oral Pathol 1979;47:120–122 [CrossRef]
- Alexandrakis G, Hubbell RN, Aitken PA. Nasolacrimal duct obstruction secondary to ectopic teeth. Ophthalmol 2000;107:189–192 [CrossRef]
|
|