Gopal Shankar Sahni1, Mahesh Prasad2.
1Department of Pediatrics, SK Medical College, Muzaffarpur, Bihar, India,
2Department of Pathology, SK Medical College, Muzaffarpur, Bihar, India.
ADDRESS FOR CORRESPONDENCE
Dr. Gopal Shankar Sahni, Department of Pediatrics, S.K.Medical College, Muzaffarpur, Bihar, India.
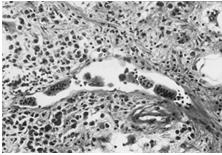
Email: dr.gopalshankar@yahoo.com.au | | Keywords | | Sinus histiocytosis with massive lymphadenopathy,emperipolesis | | | A 10 years boy presented with an insidious onset slowly increasing right sided mass in the neck for 3-4 months with appearance of similar painless swellings on the other side of the neck (Figure 1). The upper neck swellings progressed to attain the size of a 2-3cm. There was accompanying history of intermittent low grade fever associated with cough.On physical examination, he had bilateral, posterior and anterior cervical lymphadenopathy as well as submandibular lymphadenopathy which were painless, firm and non-tender. Other systems were normal. On investigation, hemogram was normal. ESR was 64 mm at end of 1 hour. Renal and liver functions were normal. Chest x-ray showed bilateral hilar lymphadenopathy. Tuberculin skin test (TST) was positive (13mm). Chest imaging studies revealed mediastinal lymphadenopathy. Ultrasound (USG) abdomen was normal. A fine needle aspiration was performed on cervical lymph nodes using a 22G needle and stained in Papanicoleau stains. The smears showed hypercellularity with abundant lymphocytes, plasma cells, neutrophils and moderate number of histiocytes. The cytoplasm of the histiocytes exhibited intact engulfed lymphocytes (emperipolesis) within them. For definite diagnosis, lymph node biopsy was performed and sections showed pericapsular fibrosis and dilated sinuses, heavily infiltrated with large histiocytes, lymphocytes and plasma cells. Histiocytes showed feature of emperipolesis, and S-100 antigen positivity on immunohistochemical stains (Figure 2). Bone marrow examination was normal. The child was given a course of antibiotics and planned for referral to higher center.
Figure 1: Cervical lymphadenopathy

Figure 2: Biopsy showing lymphophagocytosis (emperipolesis) by sinus histiocytes
Rosai-Dorfman disease (RDD) is a rare histiocytic disorder initially described as a separate entity in 1969 by Rosai and Dorfman under the term sinus histiocytosis with massive lymphadenopathy (SHML) in report of four cases that were originally diagnosed as malignant reticuloendotheliosis. (1) The disease is most common in adolescents and young adults, and is particularly found amongst the African and Caribbean population and rare in Indian population. (2) the most frequent clinical presentation of RDD is a massive bilateral and painless cervical lymphadenopathy with fever, night sweats and weight loss. Mediastinal, inguinal and retroperitoneal nodes may also be involved. Extra nodal involvement by RDD has been documented in 43% of cases with the most frequent sites being skin, soft tissue, upper respiratory tract, multifocal bone, eye and retro-orbital tissue with lymphadenopathy or as an isolated initial manifestation of disease. (2) Other reported sites include urogenital tract, breast, gastrointestinal tract, liver, pancreas and lungs. Head and neck involvement has been reported in 22% of cases, most commonly the nasal cavity followed by the parotid gland. (3) The disease is self-limiting with 70–80% undergoing spontaneous remission while other cases may be chronic with a relapsing and remitting pattern. (4) Surgery is only required when the lymph node enlargement erodes into surrounding vital organs such as heart, lungs and endocrine organs. Other therapeutic options include trials of chemotherapy with a combination of vinca alkaloids, alkylating agents and corticosteroids and or radiation therapies with variable outcome. (5) There are recent reports of cladribine (2-CdA), a purine analogue that specifically target cytokines (TNF-α and IL-6), trialed for use in recurrent RDD, providing only symptomatic relief. (6) | | | | Financial Disclosure | | None | | | | Compliance with Ethical Standards | | Funding | | None | | | | Conflict of Interest | | None | | |
- Rosai J, Dorfman RF. Sinus histiocytosis with massive lymphadenopathy. Arch Pathol1969; 87: 63-70. [PubMed]
- Foucar E, Rosai J, Dorfman RF.Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease): Review of the entity.Semin Diagn Pathol. 1990, 7:19-73. [PubMed]
- Juskevicius R, Finlay JL. Rosai-Dorfman disease of the parotid gland, cytologic and histopathologic findings with immunohistochemical correlation. Arch Pathol Lab Med.2001; 125: 1348-1350 [PubMed]
- Carbone A, Passannante A, Gloghini A, Devaney KO, Rinaldo A, Ferlito A.Review of sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease) of head and neck. Ann Otol Rhinol Laryngol. 1999, 108(11 Pt 1):1095-1104 [CrossRef]
- Antonius JI, Farid SM, Baez-Giangreco A. Steroid responsive Rosai-Dorfman disease. Pediatr Hematol Oncol. 1996; 13: 563-570. [CrossRef]
- Rodriguez-Galindo C, Helton KJ, Sanchez ND, Rieman M, Jeng M, Wang W.Extranodal Rosai-Dorfman disease in children.J Pediatr Hematol Oncol. 2004;26:19-24. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2014.60
|
| Cite this article as: | | Sahni G S, Prasad M. ROSAI-DORFMAN DISEASE. Pediatr Oncall J. 2014;11: 121-122. doi: 10.7199/ped.oncall.2014.60 |
|