Chaya A Kumar, Parul Salunke, M Mathur.
Department of Microbiology, Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai, India.
ADDRESS FOR CORRESPONDENCE
Dr Parul Salunke, 7, 2, 3, HillCrest, Bhavaninagar, Marol Maroshi Road, Andheri-East, Mumbai-400059, India.
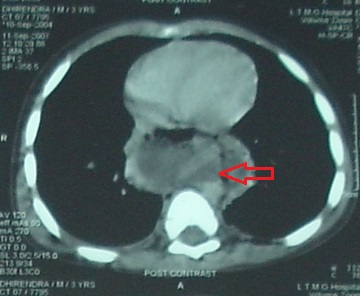
Email: parulsalunke@gmail.com | | Abstract | | Mediastinitis is a life-threatening condition generally associated with bacterial infections. Candida mediastinitis is a rare clinical entity. We report a case of a three year old male child who developed candida mediastinitis as a complication of esophageal perforation following cricopharyngoscopy. Although the polymicrobial infective agents causing mediastinitis in the present case were Klebsiella, Candida dubliniensis and C.glabrata, the patient succumbed to candidemia due to C.glabrata in spite of treatment with fluconazole. | | | | Keywords | | Candida mediastinitis, Candida glabrata, Candida dubliniensis. | | | | Introduction | | Acute mediastinitis is one of the most aggressive chest diseases. It is a life-threatening condition with a mortality rate between 14% and 42%. (1) Most cases occur as complications of cardiothoracic surgery, head and neck infections or esophageal perforation. It is generally associated with mixed bacterial infections. Fungal infections causing mediastinitis are rare. (2) Candida mediastinitis is a rare clinical entity. A case of candida mediastinitis as a complication of oesophageal perforation in a three year old child is being reported herewith. | | | | Case Report | A three year old male child was admitted at a tertiary care hospital with dysphagia and vomiting for nine months. There was history of consumption of some corrosive substance 10 months ago. An emergency tracheostomy was done at that time. He developed oropharyngeal and cricopharyngeal stenosis as a result of the corrosive poisoning. A laser excision of the cricopharyngeal stenosis was done after four months. Serial dilatations of the cricopharyngeal stenosis were performed thereafter under broad spectrum antibiotic coverage. Steroids were not administered to the patient at any time. On admission, cricopharyngoscopy was performed. This led to esophageal perforation as a complication which was confirmed on CT scan. Patient became acutely ill within 2-3 days. He developed fever with a temperature of 103oF, bounding pulse with a rate of 130/min, dyspnea with a respiratory rate of 46/min and bilateral basal crepitations. He was diagnosed as a case of acute mediastinitis. Investigations showed hemoglobin of 11.3gm %, white cell count of 28,000/cumm (polymorphs 70%, lymphocytes 30%), platelet count of 3,49,000 /cumm and normal serum electrolytes. CT scan of the chest after perforation showed ruptured esophagus with rent at C7 level and mediastinal collection with thick enhancing wall and air specks within (Figure 1). Mediastinal aspirate was collected with a sterile Ryle’s tube. The Ryle’s tube was inserted per oral and guided into the posterior mediastinum through the rent in the posterior esophagus. The pus was then aspirated using a syringe and sent for culture. A simultaneous blood culture was also collected. A feeding gastrostomy tube was inserted in view of oesophageal stenosis. Mediastinal aspirate showed plenty of pus cells, few gram negative bacilli and clusters of blastoconidia with pseudohyphae in Gram’s stain as well on potassium hydroxide (10%) mount suggestive of Candida spp. Candida dubliniensis and Candida glabrata were isolated from both oral cavity and mediastinum, whereas only C.glabrata was isolated from blood culture. Aerobically, Klebsiella pneumoniae was also isolated from oral cavity and mediastinum but not from blood culture. Child was treated with injectable cefotaxime, amikacin, vancomycin and metronidazole throughout the course of the illness. Antifungal susceptibility tests could not be done as it is not routinely performed. Injection fluconazole was started in the child. Revision of gastrostomy was attempted when the patient’s condition improved. Patient went into cardiopulmonary arrest. He was revived and put on ventilator but patient succumbed to infection and died within a week.
Figure 1: CT scan of chest - Ruptured oesophagus with a rent at C7 level, pus collection in posterior mediastinum
| | | | Discussion | Mediastinitis, the inflammation of the mediastinal tissues (3) has a range of causes including foreign body-induced esophageal perforation (4), infection of the esophagus causing esophageal rupture, pulmonary infections disseminated to mediastinum (3) and iatrogenic post-operative complications especially after cardiac surgeries. (5) Iatrogenic perforation of the esophagus is rare; however, it has a high risk of morbidity and mortality in children. It can potentially and quickly cause mediastinitis, sepsis and also multi-organ failure and even death (in 9-41% of cases) despite advanced supports in the intensive care unit. (3)
Mediastinitis is generally associated with bacterial infection. (6) Rupture and perforation of the esophagus due to the absence of serosa and having a loose areolar connective tissue allow bacteria and digestive enzymes to enter into the mediastinal and/or subphrenic spaces causing mediastinitis. (3) Gram positive organisms such as staphylococcus species account for 70-80% of cases of mediastinitis whereas mixed infection with gram positive and gram negative organisms account for approximately 40% of cases of mediastinitis. (2,3) Medical management of mediastinitis should include aggressive antimicrobial therapy with appropriate antimicrobials selected on the basis of antimicrobial susceptibility tests. Fungal agents are rarely implicated with the exception of Histoplasma capsulatum in chronic fibrosing mediastinitis. (7) Candida mediastinitis is an uncommon clinical entity. But in view of its opportunistic nature, it can emerge as a significant pathogen as seen in the present case. C.albicans has been reported in the oral cavity of 45-65% of healthy children. (8) It is most frequently implicated in oral disease in immunocompetent and immunocompromised individuals. In the present case, C.dubliniensis was isolated with C.glabrata from the oral cavity of the patient. C.dubliniensis is closely related to C.albicans in its phenotypic and genotypic characteristics. However, unlike C.albicans, it is variable in its response to commonly used antifungals like fluconazole. (9,10) Hence, it has the potential to become a common opportunistic pathogen. C.glabrata isolates are innately less susceptible to all antifungals including amphotericin B. Secondary in vitro resistance is the most common form of resistance and is most often seen for fluconazole. (11) In the present case, in spite of treatment with fluconazole, the patient developed candidemia with C.glabrata, although the patient had shown improvement initially. The management of fluconazole-resistant mucosal candidiasis is frequently unsatisfactory or short-lived, with periodic and rapid recurrences. (11)
In conclusion, C.glabrata once considered a relatively non-pathogenic saprophyte of the normal flora of healthy individuals, is now emerging as a significant nosocomial pathogen. In view of the mixed infection and high morbidity and mortality seen in mediastinitis, an early, aggressive treatment comprising of an appropriate selection of antimicrobials covering all likely pathogens, preferably after isolation, identification and antimicrobial susceptibility testing, is essential in the proper management of mediastinitis. | | | | Contributor Statement | | CA and MM did review of literature, PS did case follow up. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Macrí P, Jiménez MF, Novoa N, Varela G. A descriptive analysis of a series of patients diagnosed with acute mediastinitis. Arch Broncopneumol. 2003; 39: 428-30. [CrossRef]
- Kujath P, Schede J, Esnaashari H, Shekarriz HS, Bouchard R. Fungi in the mediastinum: rare but relevant. Mycosis 2005; 48: 18-21. [CrossRef]
- Tabari AK, Mirshemirani A, Rouzrokh M, Mohajerzadeh L, Tabari NK, Ghaffari P. Acute mediastinitis in children: a nine-year experience. Tanaffos. 2013; 12: 48-52. [PMC free article]
- Garey CL, Laituri CA, Kaye AJ, Ostlie DJ, Snyder CL, Holcomb GW 3rd et al. Esophageal perforation in children: a review of one institution's experience. J Surg Res. 2010;164:13-7. [CrossRef]
- Durandy Y. Mediastinitis in pediatric cardiac surgery: Prevention, diagnosis and treatment. World J Cardiol. 2010;2:391–8. [CrossRef] [PMC free article]
- Muellar KD. Mediastinitis. Available at URL: http://emedicine.medscape.com/article/425308-overview. Accessed on 8th April 2015.
- Kara HV, Javidfar J, Hirji SA, Balderson SS, D'Amico TA. Thoracoscopic pneumonectomy in management of histoplasmosis and fibrosing mediastinitis. Ann Thorac Surg. 2014;98:e95-6. [CrossRef]
- Akpan A, Morgan R. Oral Candidiasis. Postgrad Med J. 2002; 78: 455. [CrossRef] [PMC free article]
- Sullivan D, Clemen D. Candida dubliniensis: Characteristics and identification. J Clin Microbiol. 1998; 36: 329-334. [PMC free article]
- Sullivan D, Bennet D, Neuman H, Harwood P, Flint S, Muleahy F et al. Oligonucleotide fingerprinting of isolates of Candida species other than C.albicans and of atypical Candida species from human immunodeficiency viruses – positive and AIDS patients. J Clin Microbiol. 1993; 31: 2124-33. [PMC free article]
- Fidel PL Jr. Vazquez JA. Sobel JD. Candida glabrata: review of epidemiology, pathogenesis and clinical features with comparison to C.albicans. Clin Microbiol Rev. 1999; 12: 80-96. [CrossRef] [PMC free article]
DOI: https://doi.org/10.7199/ped.oncall.2015.37
|
| Cite this article as: | | Kumar C A, Salunke P, Mathur M. Fatal Mediastinitis Due to Candida Glabrata in a Three Year Old Child. Pediatr Oncall J. 2015;12: 80-81. doi: 10.7199/ped.oncall.2015.37 |
|