Surender Kumar1, Raktima Chakrabarti1, A S Arora2, V P Singh3, Veena Kalra4.
1Department of Pediatrics, Apollo Hospital New Delhi,
2Department of Radiology, Apollo Hospital New Delhi,
3Department of Neurosurgery, Apollo Hospital New Delhi,
4Department of Pediatric Neurology, Apollo Hospital New Delhi.
ADDRESS FOR CORRESPONDENCE
Dr. Surender Kumar, Indraprastha Apollo Hospital, Sarita Vihar, New Delhi.
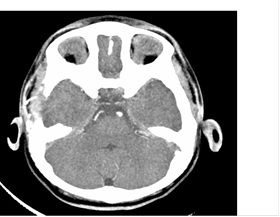
Email: drsurenderkumar97@gmail.com | | Abstract | | Moyamoya disease (MMD) is a rare cause of stroke in childhood. A high degree of suspicion is required for diagnosis as the neurological presentations are protean. Improving blood flow to hypoperfused regions by Encephaloduroarteriosynangiosis (EDAMS) has excellent results. We present 2 children who underwent surgical revascularization with EDAMS and had a good outcome. | | | | Introduction | | Moyamoya disease (MMD) is a rare progressive occlusive disease of cerebral and retinal vasculature of childhood characterized by stenosis or occlusion of the terminal portions of the intracranial internal carotid arteries and the proximal portions of the anterior / middle cerebral arteries associated with abnormal vascular networks in their vicinity visible as ‘puff of smoke’ on angiography. (1) Clinically, children present with ischemic attacks and adults with hemorrhagic events. (2-4) Surgical goal is to improve blood flow to hypoperfused cerebral regions. Encephaloduroarteriomyosynangiosis (EDAMS) has shown excellent postoperative results. (4) The natural history of untreated MMD is poor. Hence it is important to recognize and treat them early. (5) Two cases who underwent EDAMS surgery are reported. | | | | Case Report | Patient 1: A 1 year old male child was admitted with left complex partial seizure followed by persistent left hemiparesis one month ago. Twenty days later he presented to us with right sided complex partial seizure followed by mild right hemiparesis. No preceding features of increased intracranial pressure, trauma, ear discharge, recent vaccination, fever, gastrointestinal or cardiac symptoms were present. Examination revealed no neurocutaneous markers or dysmorphism. All peripheral pulses were palpable. Blood pressure (BP) was normal in all four limbs. No aortic, carotid or cranial bruit could be detected. Neurologically he was alert, conscious and oriented. Motor system revealed bilateral limb weakness (power grade 3/5 right side and 2/5 on left side). Deep tendon reflexes were exaggerated and plantars were bilaterally extensor. Cranial nerves, fundus, sensory and cerebellar systems were normal. Examination of other systems was unremarkable. Investigations including hemogram, peripheral smear, sickling test, Mantoux test, electrocardiogram (ECG), echocardiography, autoimmune workup and coagulation profile were normal. Metabolic screen (including amino acid disorders, fatty acid oxidation disorder, endocrinopathies, organic acidemias, urea cycle defect, storage disorder) were negative. Electroencephalography (EEG) showed bilateral slowing of background activity especially posteriorly with lower amplitude over left temporal region. MRI brain revealed multiple hyperintensities appearing hypointense on T1W images and hyper intense on T2W/FLAIR images in right parietal and left temporo-parietal region typical of bilateral middle cerebral artery (MCA) infarct. MR arteriogram (MRA) of brain showed long segment constriction of left MCA with lenticulostriate collaterals giving a ‘puff of smoke appearance’ suggestive of Moyamoya disease. CT brain angiography confirmed the diagnosis of Moyamoya disease (Fig 1). Bilateral EDAMS was done in two stage procedure first right sided & then left sided five months apart. Eighteen months follow up revealed no seizures, remarkable motor, speech and cognitive recovery. CT brain and MRA showed good revascularization (Fig 2).
Fig 1. Preoperative MRA brain demonstrating poor visualization of ACA, MCA on both sides with multiple collaterals in basal ganglia region with “puff of smoke” appearance
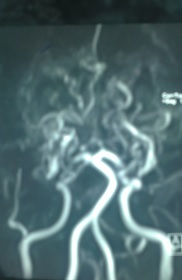
Fig 2 .Post-operative CT angiography of brain showing craniotomy with superficial temporal branch of ECA which is entering into the sylvian fissure on right side
Patient 2: A 3 years old girl with Down’s syndrome and suffering from hypothyroidism on levothyroxine supplement presented with 5 months history of recurrent right focal seizures which subsequently became left partial seizure. On examination peripheral pulses and BP were normal in all four limbs. No bruit could be detected. Neurologically she had minimal right hemiparesis. MRI brain showed multiple areas of altered signal intensity appearing hypointense on T1W images and hyper intensity on T2W/FLAIR images in both frontal regions, right parietal and left temporo-parietal region showing diffusion restriction. Multiple collaterals were seen in the perimesencephalic and both lateral cisternal regions with non-visualization of flow in distal internal carotid artery (ICA), MCA and anterior cerebral artery (ACA). MRA revealed multiple collaterals in basal region as puff of smoke appearance with non-visualized flow voids in bilateral ICA, MCA, and ACA. EDAMS was done in two stage procedure three months apart. Twenty eight months follow up revealed no seizure or stroke recurrence with good revascularization. | | | | Discussion | MMD is most prevalent in Japan, although reported globally including India. MMD, typically presents with acute cerebrovascular events - recurrent transient ischemic attacks, convulsions, migraine-like headaches and stroke in children. (1,6) Both patients presented with recurrent alternate seizures followed by hemiparesis. A high index of clinical suspicion is necessary to make the diagnosis in childhood stroke. Cerebral angiography is a basic procedure to confirm the diagnosis of MMD. Surgical revascularization procedure potentially reverses neurological deficit, prevents further ischemic seizure episodes and promotes development. The revascularization is done by direct or indirect procedure. (7) Direct revascularization method include creating actual bypass, like a superficial temporal artery-middle cerebral artery (STA-MCA) bypass that may lead to immediate improvement of symptoms; however it is technically demanding and can be associated with devastating hemorrhages. (8) Indirect methods most commonly used are encephalo-duro-arterio-synangiosis (EDAS), encephalo-myo-synangiosis (EMS) and various combinations of two (EDAMS). The other procedure includes multiple burr holes, dural inversion, galeal apposition, and omental transplant. The most extensive collateral formation was observed in the patients undergoing EDAMS. (9,10)
In adults, direct revascularization was significantly more effective than indirect revascularization (100% of patients treated with a direct bypass had a good outcome compared with 38% treated with EDAMS). In a subset of children studied, only 68% of patients had a good outcome after an STA-MCA bypass compared with 100% patients treated with EDAMS. In general pediatric cases benefit from indirect revascularization procedures. (11) In our cases, both patients underwent bilateral EDAMS in two staged procedure. Post-operative revascularization was achieved on imaging and both were seizure free with no recurrence of stroke on follow up of 18-28 months respectively. | | | | Conclusion | | A high degree of suspicion is required to diagnose MMD in children due to varied neurological presentations. Surgical revascularization with EDAMS has encouraging clinicoradiological response & should be considered as a therapeutic option in childhood. | | | | Acknowledgement | | We are thankful to the patients and all staffs of Pediatrics and Pediatric surgery and Radiology department of Apollo hospital Delhi | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Janda PH, Bellew JG, Veerappan V. Moyamoya disease: case report and literature review. J Am Osteopath Assoc. Oct 2009;109:547-553. [PubMed]
- Kuriyama S, Kusaka Y, Fujimura M, Wakai K, Tamakoshi A, Hashimoto S, et al: Prevalence and clinicoepidemiological features of Moyamoya disease in Japan: findings from a nationwide epidemiological survey. Stroke 2002; 39:42–47. [CrossRef] [PubMed]
- Kuroda S, Hashimoto N, Yoshimoto T, Iwaaki Y. Radiological findings, clinical course, and outcome in asymptomatic moyamoya disease: results of multicenter survey in Japan. Stroke. 2007; 38:1430–1435. [CrossRef]
- Kuroda S, Houkin K. Moyamoya disease: current concepts and future perspectives. Lancet Neurol. 2008; 7:1056–1066. [CrossRef]
- Yu GJ, Kim SY, Coe CJ. Moyamoya disease in Korea. Yonsei Med J. 1991;32:263-269. [CrossRef]
- Wakai K, Tamakoshi A, Ikezaki K, Fukui M, Kawamura T, Aoki R, et al. Epidemiological features of moyamoya disease in Japan: findings from a nationwide survey. Clin Neurol Neurosurg. 1997; 99 Suppl 2: S1–5. [CrossRef]
- Vilela MD, Newell DW. Superficial temporal artery to middle cerebral artery bypass: past, present, and future. Neurosurg Focus. 2008: 24(2):E2. [CrossRef] [PubMed]
- Fujimura M, Mugikura S, Kaneta T, Shimizu H, Tominaga T. Incidence and risk factors for symptomatic cerebral hyperperfusion after superficial temporal artery-middle cerebral artery anastomosis in patients with moyamoya disease. Surg Neurol 2008; 71:223-227. [CrossRef]
- Houkin K, Kuroda S, Ishikawa T, Abe H. Neovascularization after revascularization in moyamoya disease. Which technique is most useful for moyamoya disease? Acta Neurochir (Wien). 2000;142:269-76. [CrossRef]
- Kim DS, Kang SG, Yoo DS, Huh PW, Cho KS, Park CK. Surgical results in pediatric moyamoya disease: angiographic revascularization and the clinical results. Clin Neurol Neurosurg. 2007; 109:125–131. [CrossRef]
- Kinugasa K, Mandai S, Kamata I, Sugiu K, Ohmoto T. Surgical treatment of moyamoya disease: operative technique for encephalo-duro-arterio-myo-synangiosis, its follow-up, clinical results, and angiograms. Neurosurg 1993; 32:527–531. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2015.41
|
| Cite this article as: | | Kumar S, Chakrabarti R, Arora A S, Singh V P, Kalra V. Moyamoya disease - Surgical revascularization by Encephaloduroarteriosynangiosis (EDAMS). Pediatr Oncall J. 2015;12: 76-77. doi: 10.7199/ped.oncall.2015.41 |
|