Smilu Mohanlal, Jane.J.E. David, Poonam Wade, Radha Gulati Ghildiyal.
Department of Pediatrics, T.N.M.C & Nair Hospital, Mumbai.
ADDRESS FOR CORRESPONDENCE
Dr Smilu Mohanlal, A101, Deepratna, Behind HDFC bank, Juhu Versova Link Road, Andheri West, Mumbai-400053, India. Email: drsmilu@gmail.com | | Abstract | | Spontaneous pneumothorax is usually caused by asthma, staphylococcal pneumonia, cystic fibrosis in pediatric age group. The incidence ranges from 10-30%.We present an 11 month old male child with history of respiratory distress since 3 months and chest x ray suggestive of right sided pneumothorax. On treatment the child became asymptomatic, though chest x rays continued to show hyperinflation. Contrast tomography was suggestive of Swyer James syndrome. | | | | Keywords | | Spontaneous Pneumothorax, Swyer James syndrome | | | | Introduction | | Swyer-James-McLeod Syndrome (SJMS) is an uncommon, emphysematous disease characterized by radiologic hyperlucency of pulmonary parenchyma due to loss of the pulmonary vascular structure and to alveolar overdistension. (1) Swyer James syndrome is diagnosed by exclusion of other causes of unilateral hyperlucency as this particular finding correlates with several diseases of either the lung parenchyma or vasculature. Parenchymal diseases include congenital lobar emphysema, bronchogenic cyst, pneumatocele, bronchiectasis with air trapping and emphysema secondary to bronchospasm. Congenital vascular disorders such as pulmonary artery agenesis or hypoplasia are the differentials for the condition. (2) We present an 11 months old boy with left sided pneumothorax due to SJMS. | | | | Case Report | An 11 months old male child presented with respiratory distress for 3 months which were relieved temporarily with bronchodilator nebulizations. There was no fever or history suggestive of foreign body ingestion. No investigations had been done in the past 3 months. His immunization was upto date as per EPI schedule. On admission the child weighed 8.5 kg (between 3rd and 50th percentile), length was 71 cms (3rd and 50th percentile) and head circumference was 44 cms (3rd and 50th percentile). He was tachypneic and had intercostal and subcostal retractions with decreased air entry in the left lung field. Other systems were normal. Chest x ray and CT scan of chest showed left sided pneumothorax. (Fig 1 and 2). Investigations showed a hemoglobin of 9.9 gm%, white blood cell count of 14,300/cumm and platelets of 3,70,000 cells/cumm. Arterial blood gas showed pH of 7.339, PO2 of 72, PCo2 of 42.8 and oxygen saturation of 90 mm of Hg. ESR was 20 mm/hr. Gastric lavage for acid fast bacillus and Mantoux test were negative. Blood culture did not grow any organism. An intercostal drain (ICD) was inserted for 72 hours. Post ICD removal the child was stable and discharged after 48 hours. On follow up child was asymptomatic. Chest x ray showed a left sided hyperinflation. CT scan and serial chest X rays evaluation revealed Swyer James Macleod syndrome (Fig 3). Child is on regular follow up with us and is asymptomatic.
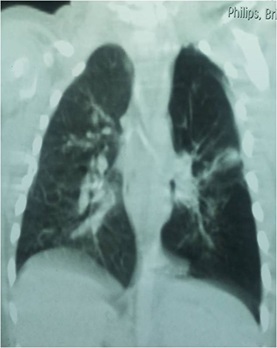
Figure 1: Chest X ray showing left sided pneumothorax

Figure 2: CT Scan showing Left sided Pneumothorax
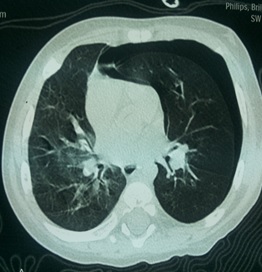
Figure 3a: Chest X-ray showing left sided hyperlucency- a feature of Swyer James Syndrome

Figure 3b: CT scan chest showing left sided hyperlucency- a feature of Swyer James Syndrome
| | | | Discussion | | SJMS is an uncommon disorder. Among 52 patients with bronchiolitis obliterans, Go sink et al. (3) reported only two cases of hyperinflation. The diagnosis is usually based on radiologic and clinical findings rather than on the results of pathologic examination. SJMS is characterized by the presence of constrictive bronchiolitis with dilatation and destruction of alveolar structures, resulting in significant air trapping and lung. Although classically involving an entire lung, the disorder can be lobar or segmental. The main pathogenetic event seems to be acute bronchiolitis with obliteration of small airway in infancy or early childhood. The disease starts as an obliterative bronchiolitis with concomitant vasculitis commonly following infections with certain organisms. Consequent damage to the terminal or respiratory bronchioles in early childhood prevents normal development of their alveolar buds. (4) Respiratory infections associated with bronchiolitis obliterans and the manifestation of SJMS include measles, whooping cough by bordetella pertussis, tuberculosis, mycoplasma pneumonia, influenza A and adenoviral infections with the subtypes 3, 7, and 21. (5) The onset of symptoms typically occurs during infancy or early childhood in association with frequent respiratory infections. Patients present usually with productive cough, shortness of breath, and dyspnea on exertion. CT scan showing features of air trapping is the modality of diagnosis. Other investigations include ventilation perfusion scanning and CT angiography. (6) Treatment is primarily conservative and supportive with the use of antibiotics and bronchodilators, surgical intervention is required in patients presenting with recurrent infections not improving with conservative support, patients with clinical deterioration and resulting failure to thrive and finally those presenting with spontaneous or recurrent pneumothorax. (7,8) | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Reid L, Simon G. Unilateral lung transradiancy. Thorax 1962, 17:230–239. [CrossRef]
- Fregonese L, Girosi D, Battistini E, Fregonese B, Risso FM, Bava GL, et al. Clinical, physiologic, and roentgenographic changes after pneumonectomy in a boy with Macleod/Swyer-James syndrome and bronchiectasis. Pediatr Pulmonol 2002;34:412–416. [CrossRef] [PubMed]
- Gosink BB, Friedman PJ, Liebow AA. Bronchiolitis obliterans. Roentgenologic- pathologic correlation. AiR 1973, 117:816–832.
- Erkasar CF, Caglar CE, Koray D, Ilgin KN. Bilateral Swyer-James (Macleod's) syndrome. Indian J Pediatr. 2002, 68:433–435. [CrossRef]
- Schlesinger C, Veeraraghavan S, Koss MN: Constructive (obliterative) bronchiolitis. Curr Opin Pulm Med. 1998, 4:288–293. [CrossRef] [PubMed]
- O'Dell CW, Taylor A, Higgins CB, Ashburn WL, Schillaci RF, Alazraki NP. Ventilation-perfusion lung images in the Swyer-James syndrome. Radiology 1976, 121:423–426. [CrossRef] [PubMed]
- Lucaya J, Gartner S, García-Peña P, Cobos N, Roca I, Liñan S. Spectrum of manifestations of Swyer-James-MacLeod syndrome. J Comput Assist Tomogr. 1998, 22:592–597. [CrossRef] [PubMed]
- Marchevsky AM et al: Swyer-James (MacLeod) syndrome with placental transmogrification of the lung: a case report and review of the literature. Arch Pathol Lab Med 2005, 129:686–689. [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2015.55
|
| Cite this article as: | | Mohanlal S, David J, Wade P, Ghildiyal R G. A Case of Spontaneous Pneumothorax-Swyer James Syndrome. Pediatr Oncall J. 2015;12: 110-111. doi: 10.7199/ped.oncall.2015.55 |
|