Kamel Abidi, Mohamed Riadh Boukhris, Manel Jallouli, Yousra Hammi, Ouns Naija, Tahar Gargah.
Nephropediatric department, Charles Nicolle Hospital, Tunisia.
ADDRESS FOR CORRESPONDENCE
Dr. Kamel Abidi, Nephropediatric department, Charles Nicolle Hospital. Boulevard 9 Avril, Bab Souika, 1006 Tunis, Tunisia.
Email: abidikamel8@yahoo.fr | | Keywords | | Aspergillus Flavus, child, microangiopathy, renal transplantation. | | | A 17-year-old boy with end stage renal disease received a renal transplant from a deceased donor. Both donor and recipient were negative for cytomegalovirus (CMV) infection. His past medical history included end stage renal disease due to Alport syndrome. Haemodialysis through an arteriovenous fistula was given for 4 years and 9 months prior to transplant. The initial immunosuppression post-transplant consisted of quadruple therapy including: corticosteroids, mycophenolate mofetil, induction with thymoglobulin and delayed use of tacrolimus. Anti-infectious prophylaxis with cotrimoxazole was prescribed. Antithrombotic prophylaxis with low-molecular-weight heparin was used. The early postoperative course was uncomplicated. The patient was transferred to our department from urology unit, 7 days after transplantation on tacrolimus 6 mg/day, prednisone 60mg/day and mycophenolate mofetil 2g/day. His urine output was estimated at 3 liters/day. The serum creatinine level was 320µmol/l. Three days later, he suddenly developed dyspnea with severe hypoxemia and massive hemoptysis. Chest X-ray revealed diffuse pulmonary interstitial infiltrate without cardiomegaly or pleural effusion. Computerized tomography scan confirmed the chest X-ray findings (fig1). He developed respiratory failure and needed mechanical ventilation. Bronchoscopy and bronchial biopsy revealed aspergillus flavus growing in mucosa. He was started on intravenous voriconazole to which he had a good response. Concerning the allograft function, the patient developed oligo-anuria and increasing serum creatinine. Renal graft biopsy performed two weeks after transplantation, revealed diffuse glomerular injury with capillary thrombosis and marked tubulointerstitial injury. All immunosuppressive medications were stopped. Patient was detransplanted and he returned to dialysis. The general condition of the patient improved and he was extubated after 2 weeks of mechanical ventilation. After 6 months of treatment, the patient is asymptomatic, his chest X-ray is without abnormalities.
Fig 1: chest computerized tomography showing diffuse pulmonary interstitial infiltrates.
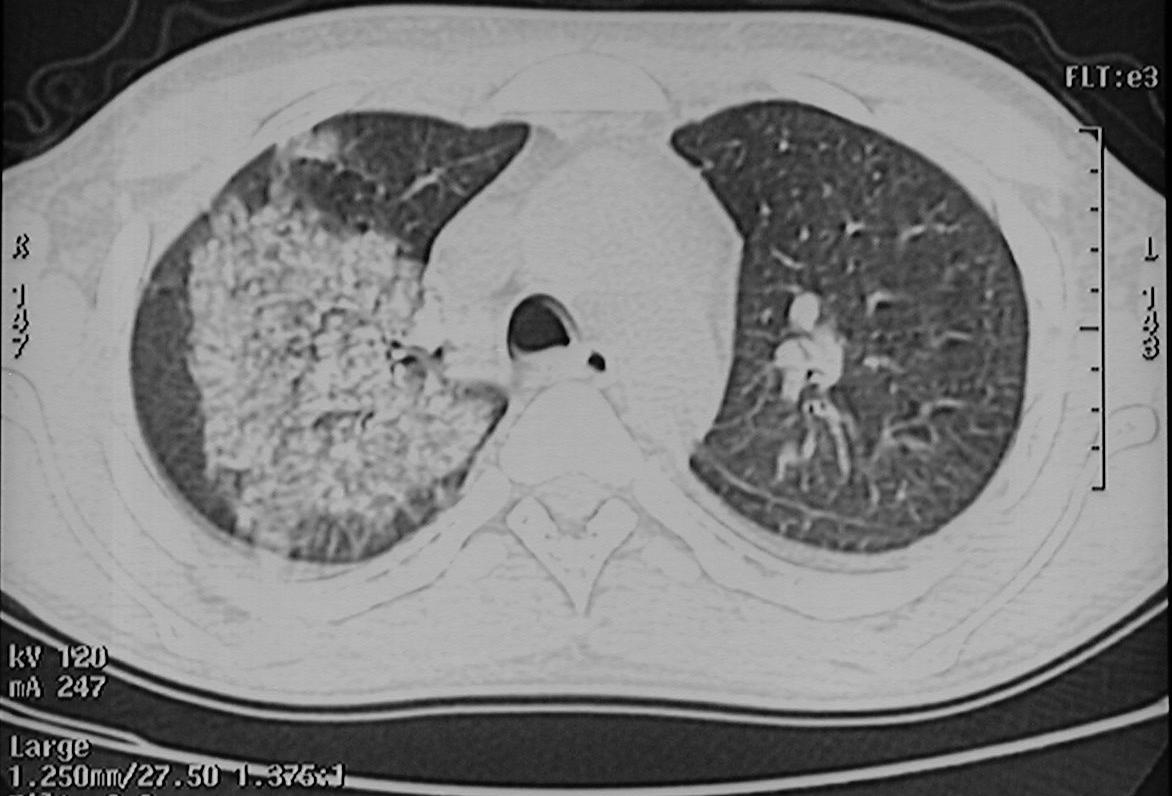
Multiple organ transplantation and immunosuppressive therapy have increased the risk of developing fungal infections in transplant patients. Aspergillus infection occurs mainly after lung and bone marrow transplantation. However it’s uncommon in pediatric renal transplant recipients. (1,2) Our patient is the first Tunisian reported case. The onset of the invasive aspergillosis is usually late, estimated in the study of Hoyo about 217 days from renal transplantation. (3) In our case, the onset of the infection is extremely precocious, about 10 days after renal transplantation. The aspergillus involves primarily the lungs, followed by the skin, sinus and finally central nervous system. (4,5) Clinical presentation in our patient was relatively evocative because of hemoptysis, severe hypoxia and sepsis. Aspergillus invades blood vessel and progresses across tissue. Bronchoscopy done in patients with aspergillus tracheobronchitis shows a whitish membrane at times almost completely covering the entire mucosa and often obstructing the airway. The specificity of a positive result of the examination of the bronchoalveolar lavage fluid is almost 97% but the sensitivity is 30 to 50%. (5) The most typical CT finding of invasive pulmonary aspergillosis is the presence of nodules or the air crescent sign and often parenchymal infiltrates as seen in our patient. (4) Concomitant thrombotic microangiopathy has only been reported in adult recipients and most often leads to graft loss. (3) The mortality rate in transplant recipients with invasive aspergillosis is very high. (1) However, early diagnosis and treatment can improve the prognosis. Our early diagnosis and rapid initiation of appropriate treatment saved the patient's life but the thrombotic microangiopathy led to loss of the graft.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Pérez-Sáez MJ, Mir M, Montero MM, Crespo M, Montero N, Gómez J, et al. Invasive aspergillosis in Kidney transplant recipients : a cohort study. Exp Clin Transplant. 2014 Apr; 12:101-5. [PubMed]
- Zhang XD, Hu XP, Yin H, et al. Aspergillus pneumonia in renal transplant recipients. Chin Med J 2008; 121:791-4. [CrossRef]
- Hoyo I, Sanclemente G, de la Bellacasa JP, Cofán F, Ricart MJ, Cardona M, et al. Epidemiology, clinical characteristics, and outcome of invasive aspergillosis in renal transplant patients. Transpl Infect Dis 2014; 16:951-7. [CrossRef]
- Burgos A, Zaoutis TE, Dvorak CC, et al. Pediatric invasive aspergillosis: a multicenter retrospective analysis of 139 contemporary cases. Pediatrics 2008; 121:1286-94. [CrossRef]
- Ardalan MR, Ansarin K, Hejazi E, et al. Aspergillosis after renal transplantation. Saudi J Kidney Dis Transpl 2005; 16:330-3. [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2015.48
|
| Cite this article as: | | Abidi K, Boukhris M R, Jallouli M, Hammi Y, Naija O, Gargah T. Invasive Aspergillosis with Thrombotic Microangiopathy in a Pediatric Renal Transplant Recipient. Pediatr Oncall J. 2015;12: 85-86. doi: 10.7199/ped.oncall.2015.48 |
|