Sandip Bartakke1, Nakul Pathak2, Shrividya S3.
1Department of Clinical Hematology, Aditya Birla Memorial Hospital, Pune, India,
2Department of Pediatrics, Aditya Birla Memorial Hospital, Pune, India,
3Department of Pathology, Aditya Birla Memorial Hospital, Pune, India.
ADDRESS FOR CORRESPONDENCE
Dr Sandip Bartakke, Aditya Birla Memorial Hospital, Chinchwad, Pune. PIN 411033. Email: spbartakke@gmail.com | | Abstract | | Kikuchi-Fujimoto disease is a self-limiting disease which frequently appears as fever with lymphadenopathy, thus creating the need for differential diagnosis with lymphoma, systemic lupus erythematosus {SLE}, infectious mononucleosis, cat-scratch disease, and toxoplasmosis. However, there are cases in which it may evolve with complications such as aseptic meningitis, cerebellar ataxia, and aseptic myocarditis. We report a case of a 14-year-old boy who presented with fever and lymphadenopathy. Kikuchi disease was diagnosed on the basis of lymph node histopathology. He developed hypotension requiring fluid bolus and inotropic support with electrocardiogram suggestive of myocarditis. There was significant improvement of the clinical picture with prednisolone. | | | | Keywords | | Kikuchi Fujimoto Disease, Myocarditis | | | | Introduction | | Kikuchi-Fujimoto disease (KFD) is a rare, usually self-limiting disease that was originally reported in patients of Asian heritage. Cases are now described in all ethnic groups. (1) The etiology of the disease is unknown, although viral and bacterial causes have been suggested. The disease most commonly occurs in people younger than 40 years of age. (2) The characteristic clinical presentation of the disorder includes cervical lymphadenopathy and prolonged fever but the presentation may be variable. Its natural course is usually benign and the clinical symptoms and signs disappear within a few months without any specific treatment. Correct diagnosis requires a histopathologic examination by lymph node biopsy. Kikuchi Fujimoto disease is usually a benign disease. However patients may have severe systemic complications in the form of aseptic meningitis, cerebellar ataxia, aseptic myocarditis, panuveitis, and acute renal failure. (3-7) Here we present a case of KFD with possible myocarditis. | | | | Case Report | A 14-year-old male child presented with cough, cold and fever for 15 days. There was no history of contact with patient having tuberculosis, weight loss, respiratory distress, otorrhoea or rash. The patient had received anti-malarial treatment with a 7-day course of antibiotics along with oseltamivir, but there was no response. On examination, there was pallor. Rest of the examination was normal. Investigations showed microcytic hypochromic anemia with hemoglobin of 8.6 gm/dL, white cell count of 4,300cells/cumm (62% polymorphs, 27% lymphocytes, and 8% monocytes), and platelet counts of 489,000 cells/cumm. ESR was elevated (67 mm/h) as was serum procalcitonin (7.21 mcg/L). Renal and liver function tests, serum LDH and uric acid were normal. Blood culture reports (2 samples 3 days apart) did not show any growth. Serological studies for Epstein Barr virus (EBV), Brucella, HIV, HBsAg and scrub typhus were negative. ANA was also negative. Urine studies including culture were also normal. Bone marrow aspiration and biopsy was normal. Bone marrow culture did not reveal any growth. Radiological investigations – chest X-ray, ultrasound of abdomen and echocardiography were normal with left ventricular ejection fraction (LVEF) being 60%. During the second week of admission, patient developed small cervical lymphadenopathy measuring 1.5 by 1 cm and he continued to have fever. Computerized tomography scans of chest and abdomen were done. These revealed prominent bilateral axillary lymphadenopathy 1.5 by 1.7 cm with inguinal and mesenteric lymphadenopathy – largest being 3.5 by 3.7 cm in right iliac fossa (RIF). Cervical lymph node biopsy (FIG. 1) revealed large circumscribed area of necrosis extending to the capsule. The necrotic areas showed eosinophilic debris, abundant apoptosis and macrophages surrounded by histiocytes, immunoblasts, eosinophils and lymphocytes. Immunohistochemistry showed mainly CD 68 positive macrophages. This picture was consistent with diagnosis of KFD. Patient had 2 episodes of hypotension which required fluid boluses and low dose inotropic support – dopamine at 10 mcg/kg/min for about 36 hours and then tapered off on 2nd day. For these episodes, ECG was done which showed sinus tachycardia, diminished QRS voltages, and non-specific ST and T-wave changes suggestive of myocarditis. However, serum creatinine kinase MB (CPK- MB) was 9 U/L. Echocardiography done at this time showed LVEF to be 50%. Patient was treated with low dose steroids (prednisolone 1mg/kg) for 1 week and the dose was tapered off over next week. Patient became afebrile 24 hours after starting steroids and inotropic support was tapered off in 2 days. On follow up at 6 months, he remains well without any symptoms or lymphadenopathy.
Figure 1: Histopathology of lymph node suggestive of Kikuchi-Fujimoto
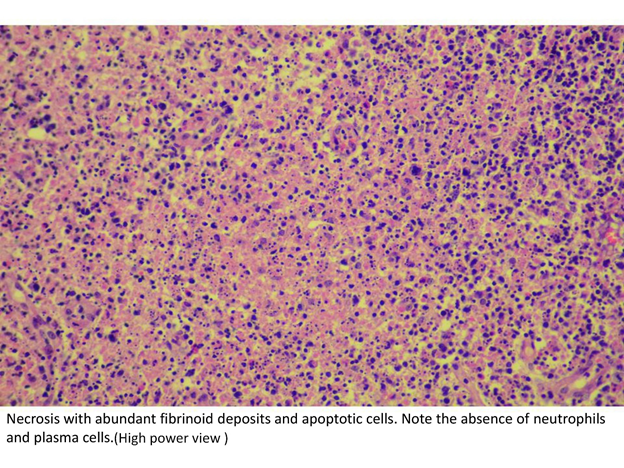
| | | | Discussion | | KFD is a disease of acute or sub acute onset, which evolves over a period of 2-3 weeks. The course is self limited. Typical presentation is cervical lymphadenopathy (56-98 % of cases), often unilateral (88.5%) with tenderness (59%) and frequently located in the posterior cervical triangle (88.5%). (8) Our patient was a male who presented with fever of unknown origin (FUO) and developed lymph nodes after 2 weeks of illness. Although there are no specific diagnostic tests for KFD, the diagnosis is usually made based on histopathologic findings from an excision biopsy of the involved node. Laboratory results usually yield normal results, but a few patients may have elevated ESR mild anemia and leucopenia. (9) Our patient had elevated ESR, anemia and leucocytopenia as well. The histopathologic features include necrotic changes with karyorrhexis and infiltration by histiocytes and plasmacytoid monocytes. (2) The clinical and histological features of KFD may mimic diseases like lymphomas, SLE, metastatic adenocarcinomas, Kawasaki’s disease, mononucleosis, herpes infections and tuberculosis. Differentiation can be challenging. It is speculated that KFD may be under-diagnosed in clinical practice, as many mild forms with low grade fever and small cervical lymphadenopathy without biopsies may have been wrongly diagnosed as viral infections. (10) KFD must be considered in the differential diagnosis in patients with fever, unilateral cervical adenopathy, and histological features showing large necrotic foci with evidence of apoptosis and infiltration by histiocytes. Recognition of KFD will avoid misdiagnosis. Supportive measures are the mainstay of therapy as no treatment is required in most cases of KFD. However patients may have severe systemic complications in the form of aseptic meningitis, cerebellar ataxia, aseptic myocarditis, panuveitis, and acute renal failure. (3-7) In our patient, there were 2 episodes of hypotension with ECG changes suggestive of myocarditis, although enzymes remained in normal range. Thus KFD may have systemic manifestation which might require treatment as well. | | | | Conclusion | | As KFD is rare, a high level of awareness is needed to suspect the diagnosis. KFD should be kept in the differential diagnosis of FUO and cervical lymphadenopathy in children. Confirming the diagnosis early helps in the timely institution of proper management. Systemic manifestations should be looked for especially in sick children. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Tower RL II, Camitta BM. Kikuchi Fujimoto Disease. In: Kliegman RM et al. Nelson Textbook of Pediatrics. 19th ed. Philadelphia. Elsevier Saunders. 2011: 1724.
- Tsang WVW, Chan JKC, Ng CS. Kikuchi's lymphadenitis: a morphologic analysis of 75 cases with special reference to unusual features. Am J Surg Pathol. 1994; 18: 219–231. [CrossRef] [PubMed]
- Calvo Romero JM. Enfermedad de Kikuchi-Fujimoto (linfadenitisnecrotizantehistiocitaria). Rev Clin Esp. 2002; 202:94-95. [CrossRef]
- Pérez Alvarez MJ, Moreno López M. Panuveitis as a possible ophthalmic complication of Kikuchi-Fujimoto disease.Arch Soc Esp Oftalmol. 2005; 80:41-4. [PubMed]
- Silva AF, Focaccia R, Oliveira AC, Sementilli A, Reis GF. Kikuchi-Fujimoto disease: an unusual association with acute renal failure. Braz J Infect Dis. 2010; 14:621-627. [CrossRef] [PubMed]
- Chan JK, Wong KC, Ng CS. A fatal case of multicentric Kikuchi's histiocytic necrotizing lymphadenitis. Cancer.1989; 63:1856-62.
- Chang KT, Lin HY, Kuo CH, Hung CH. A Case of Kikuchi–Fujimoto Disease Presenting with Shock. Tungs' Medical Journal.2014;8:42-44.
- Bosch X, Guilabert A, Miquel R, Campo E. Enigmatic Kikuchi-Fujimoto disease: a comprehensive review. Am J Clin Pathol. 2004; 122:141–152. [CrossRef] [PubMed]
- Bosch X, Guilabert A. Kikuchi-Fujimoto disease. Orphanet J Rare Dis. 2006;1. [CrossRef]
- Kuo TT. Kikuchi's disease (histiocytic necrotizing lymphadenitis). A clinicopathologic study of 79 cases with an analysis of histologic subtypes, immunohistology, and DNA ploidy. Am J Surg Pathol.1995;19:798– 809. [CrossRef] [PubMed]
DOI: https://doi.org/10.7199/ped.oncall.2016.3
|
| Cite this article as: | | Bartakke S, Pathak N, S S. A Case Report of Kikuchi Fujimoto Disease with Myocarditis. Pediatr Oncall J. 2016;13: 19-20. doi: 10.7199/ped.oncall.2016.3 |
|