Deepali Ambike, Abhijeet Byale, Rijwana Sayyad, Vinit Rathod, Komal Bijarniya.
Department of Pediatrics, Post Graduate Institute- Yashwantrao Chavan Memorial Hospital, Pune, Maharashtra, India.
ADDRESS FOR CORRESPONDENCE
Dr Deepali Ambike, Professor & Head, Pediatrics, Post Graduate Institute- Yashwantrao Chavan Memorial Hospital, Pimpri, Pune-18, Maharashtra, India.
Email: ambikedeepa@gmail.com | | Keywords | | Cloacal exstrophy, exstrophy of the bladder, omphalocele | | | A 22-year-old pregnant female presented at 39.1 weeks of gestation in third stage of labour with hand prolapse to our emergency department. She immediately underwent emergency lower segment caesarean section (LSCS). There was no significant antenatal history of exposure to teratogenic drugs or radiation, infection, diabetes mellitus or hypertension. There was no history of treatment for infertility. No antenatal registration or antenatal scan was done. She delivered a live baby weighing 2.8 kg with head circumference of 34.5 cm, who had multiple congenital abnormalities. There was no history of consanguinity or similar malformations in previous deliveries. There was presence of omphalocele, exstrophy of bladder, imperforate anus, and genital anomalies (Figure 1 and 2) along with bilateral congenital talipes equinovarus (CTEV) and lumbosacral meningocele.
Figure 1. Exstrophy of bladder, omphalocele along with imperforate anus.
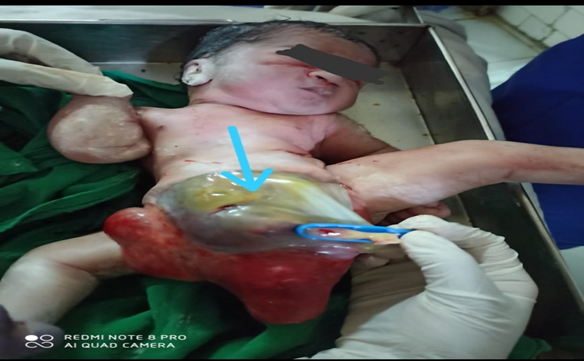
Figure 2. Absent Genitalia.

X-ray thoracolumbar spine lateral view showed lumbosacral meningocele. Diagnosis of OEIS complex was made. Ultrasound (USG) of the abdomen and pelvis confirmed OEIS but the gender could not be evaluated due to obscure genital organs. Chromosomal analysis could not be done as the parents financial status did not permit for any future work up and intervention. The neonate died on day 5 of life.
OEIS complex is a severe form of exstrophy-epispadias complex which results from improper closure of ventral abdominal wall due to failure of cephalocaudal and lateral folding with associated defects of cloaca and urorectal septum.1 The term OEIS complex was proposed to describe findings by Carey et al based on a retrospective search of medical records of 175 infants and has been described in the literature and is regarded as an entity.2 The incidence is one in 200,000 to 400,000 pregnancies.3 OEIS complex results from developmental defects affecting the mesenchyme, which is required for the development of infraumbilical mesoderm, the urorectal septum and lumbosacral somites. Therefore, any abnormality in mesodermal migration leads to premature rupture of cloacal membrane leading to omphalocele and exstrophy of cloaca.3 Abnormalities of urorectal septum led to persistent cloaca and imperforate anus.3 Genital anomalies are due to the failure of fusion of genital tubercles and separation of pubic rami.3 Association of OEIS with deletion of chromosome 1p36 has been reported and also with maternal exposure to diazepam, cigarette smoking, and maternal obesity.4 We could not elicit such a history in our patient. Additional malformations reported include rib anomalies, abnormal ears, hydrocephaly, microcephaly, encephalocele, cardiac defects, trachea-oesophageal fistula, and oesophageal atresia.5 Microcephaly with head circumference less than 10th percentile was noted in our patient. An early antenatal diagnosis and urgent surgical correction is crucial in the management. The mother of our patient was not registered for antenatal care at any hospital; neither any obstetrics scan was done throughout the pregnancy. She did not receive periconceptional folic acid supplementation which is recommended by World Health Organization (WHO) to prevent neural tube defects in fetus.
| | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Carey JC, Greenbaum B, Hall BD. The OEIS complex (omphalocele, exstrophy, imperforate anus, spinal defects). Birth Defects Orig Artic Ser. 1978;14:253 263.
- Haldar A, Sharma AK, Phadke SR, Jain A, Agarwal SS. OEIS complex with craniofacial anomalies - Defect of blastogenesis? Am J Med Genet. 1994;53:21 23. [CrossRef] [PubMed]
- Kar A, Kar T, Dnal I, Biswal P, Jena S. Perinatal autopsy finding in OEIS complex associated with other congenital anomalies. Int J Sci Res. 2014;3:2039-2041.
- El-Hattab AW, Skorupski JC, Hsieh MH, Breman AM, Patel A, Cheung SW, et al. OEIS complex associated with chromosome 1p36 deletion: A rare case report and review. Am J Med Genet A. 2010;152A:504-511. [CrossRef] [PubMed]
- Smith NM, Chambers HM, Furness ME, Haan EA. The OEIS complex (omphalocele-exstrophy-imperforate anus-spinal defects): Recurrence in sibs. J Med Genet. 1992; 29:730-732. [CrossRef] [PubMed] [PMC free article]
DOI: https://doi.org/10.7199/ped.oncall.2021.32
|
| Cite this article as: | | Ambike D, Byale A, Sayyad R, Rathod V, Bijarniya K. A Rare Case of Omphalocele, Exstrophy of Bladder, Imperforate Anus and Spinal Defect Complex with Genital Anomalies in a Term Neonate. Pediatr Oncall J. 2021;18: 93-94. doi: 10.7199/ped.oncall.2021.32 |
|